ARCHIVE
When people are seriously hurt in horrific car accidents, burned in fires, or injured in violent crimes, first responders rush in to treat injuries and to offer emotional support. But who provides support to the first responders? Repeated exposure to gruesome injuries or loss of life can lead to emotional trauma for these everyday heroes.
It is estimated that 1 in 10 first responders will develop a trauma-related problem. And this puts firefighters, law enforcement personnel, paramedics, and others at increased risk of anxiety, depression, substance abuse, marital conflict, sleep disturbances, trouble concentrating, anger, and suicide. It is estimated that 30% of first responders will develop mental health conditions compared to 20% of the civilian population.
In addition, first responders are more likely to die by suicide than in the line of duty, according to the Ruderman White Paper on Mental Health and Suicide of First Responders. This study reported that in 2017, 140 police officers and 103 firefighters died by suicide compared to 129 police officers and 93 firefighters who died on the job. However, the research suggests that not all suicides are reported, so the numbers could be even higher.
What Brain Imaging Reveals about Suicide
Amen Clinics has done brain imaging studies on more than 300 people, including some first responders, who have attempted to take their own life. Some of the common traits found in these people include past head injuries, exposure to trauma, impulsivity, anger, and negativity.
- Concussions and traumatic brain injuries (TBIs): First responders are at heightened risk of head injuries due to falls, blows to the head, vehicle collisions, exposure to explosions, and more. A 2018 study in JAMA shows that people with a TBI are nearly twice as likely to take their own life compared with those who have no history of head trauma. At Amen Clinics, 40% of the people we see have evidence of past head trauma on SPECT scans even if they don’t recall having experienced a concussion or TBI.
- Exposure to trauma: People who have been exposed to trauma and those who have post-traumatic stress syndrome (PTSD) are at a higher risk of suicide. Brain imaging studies on over 1,000 patients with PTSD demonstrates increased activity in the limbic system (the brain’s emotional center), basal ganglia (the brain’s anxiety center), and anterior cingulate gyrus (the brain’s gear shifter that helps you go from thought to thought) in what looks like a diamond pattern. In 2005, Amen Clinics evaluated and treated 6 police officers who had been involved in on-the-job shootings, developed PTSD and were placed on medical leave. The “diamond pattern” was seen in all of their brain scans.
- Impulsivity: The area of the brain that is involved in impulse control is called the prefrontal cortex (PFC). When there is low blood flow to the PFC, it increases impulsivity. Suicide is considered an impulsive act.
- Anger: Irritability, aggression, and violence—traits associated with suicide—are commonly seen in people who have abnormal activity in the temporal lobes. An Amen Clinics study found that 62% of patients with suicidal thoughts or a past attempt showed abnormal activity in the left temporal lobe.
- Getting stuck on negative thoughts: Some people may fleetingly think that the world would be a better place without them in it. But they quickly move on from that thought. In people who make suicide attempts, they are generally unable to stop these thoughts from looping inside their heads. This is often seen in people who have too much activity in the anterior cingulate gyrus (ACG).
Change Your Brain, Heal Your Mind
The good news is you are not stuck with the brain you have. You can make it better. If you’ve had a head injury and been exposed to trauma, or if you struggle with impulsiveness, anger, or negative thinking, there are numerous therapies that can help you change your brain and heal your mind.
- Healing head trauma: People with head trauma have shown great benefit from therapies called neurofeedback and hyperbaric oxygen therapy (HBOT). In addition, it’s important to have hormone levels tested as they are often low in people with head injuries.
- Soothing trauma and PTSD: The 6 police officers suffering from PTSD underwent a special psychotherapeutic technique called EMDR (eye movement desensitization and reprocessing). All of the officers reported significant improvement and went back to work. Their follow-up scans showed calming of the overactive areas.
- Controlling impulsivity: There are many solutions to improve blood flow to the PFC to boost impulse control. A higher protein, lower carbohydrate diet tends to help, as does physical exercise and certain stimulating supplements, such as green tea, rhodiola, and ginseng.
- Taming anger: To support temporal lobe activity, natural supplements such as GABA, magnesium, theanine, and taurine have been found to be helpful. Neurofeedback also enhances temporal lobe functioning.
- Getting unstuck: Optimizing the ACG involves training the brain to become more flexible and see options and new ideas. The supplements 5-HTP, saffron, and St. John’s wort are the most helpful to calm the ACG. In addition, learning to recognize when you’re getting stuck and distracting yourself is a helpful technique.
Our first responders deserve more support. Helping them understand that “mental health” problems are really “brain health” problems is an important step in ending the stigma associated with seeking treatment. Thinking of these issues as biological rather than psychological may encourage more of these heroes to get the help they need so that heartbreaking suicides may be prevented.
If you are having suicidal thoughts, call the National Suicide Prevention Lifeline at 1-800-273-TALK (8255).
At Amen Clinics, we have treated hundreds of people who have attempted suicide, including first responders, and many more who have considered taking their own life. We use brain SPECT imaging to help identify underlying brain abnormalities that increase the risk of suicide and offer personalized treatment plans to optimize the brain so you can have a healthier outlook on life.
If you or a loved one is experiencing suicidal tendencies and would like more information on how to heal your brain and save a life, call us at 888-288-9834 or schedule a visit online.
Firefighters routinely put themselves in harm’s way by battling urban blazes and wildfires. But the flames aren’t the only danger they face. Breathing in carbon monoxide and other toxins, repeated exposure to emotional trauma, and the possibility of head injuries put them at increased risk of unhealthy brain function.
Brain imaging studies on a group of 50 of firefighters performed at Amen Clinics show troubling findings:
- 67% show evidence of head trauma
- 63% show evidence of moderate toxicity
- 45% show evidence of chronic emotional trauma
- 40% show evidence of ADHD
All of these brain issues increase the likelihood of mental, behavioral, and cognitive problems, but few firefighters are aware of this.
How Head Injuries Cause Lasting Harm
Falling off the ladder, structure collapse, traffic collisions involving emergency vehicles—firefighters are at risk for head trauma. It is estimated that up to 15% of all firefighter injuries are head injuries. That amounts to over 4,000 head injuries a year, and the number could actually be much higher since many first responders may not think their injury is significant enough to report.
But concussions and traumatic brain injuries (TBIs)—even if they don’t cause you to lose consciousness—can lead to problems in the following weeks, months, and years. Research shows that head trauma increases the risk of depression, anxiety and panic disorders, ADD/ADHD, drug and alcohol abuse, psychosis, chronic emotional trauma and stress, borderline and antisocial personality disorders, dementia, and suicide. But since psychiatrists rarely look at the organ they treat, first responders may not be aware that this is the root cause of their issues.
When Toxins Attack the Brain
Firefighters can be exposed to many toxins, including carbon monoxide, benzene, asbestos, and diesel exhaust. Statistics from a 2018 report from the National Fire Protection Association show that there were an estimated 44,530 exposures to hazardous conditions, such as radioactive materials, chemicals, and fumes.
There is growing concern that exposure to such chemicals is increasing rates of cancer among first responders. But this exposure poses another dangerous threat that isn’t getting enough attention—toxic brain.
The brain is the most metabolically active organ in the human body. As such, it is extremely vulnerable to damage from toxins, and having a toxic brain is linked to depression, ADD/ADHD, learning problems, memory problems, brain fog, autism, temper outbursts, psychotic behavior, and suicide.
On brain SPECT scans, which measure blood flow and activity in the brain, a toxic brain looks like a “Swiss cheese” brain that is full of holes. The “holes” reflect areas with low blood flow and are a sign of an unhealthy brain. It looks like their brains have been poisoned.
How Exposure to Trauma Affects the Brain
First responders witness some horrific incidents, but “they’re actually trained to stuff it, to push it down,” according to Dr. Nancy Bohl-Penrod, a psychotherapist and trainer to first responders. In an episode of The Brain Warrior’s Way podcast, Bohl-Penrod said their training dictates, “Don’t let it bother you. Get over it as quickly as you can, because you’re going to go on another call.” In response to the repeated exposure to trauma, she’s seen firefighters develop mild depression, become more short-fused, turn to alcohol, and withdraw from their families.
These issues are related to abnormal activity in the brain. Brain imaging scans show that chronic exposure to trauma is associated with overactivity in the emotional brain, which is known as the limbic system. When there is too much activity in this brain region, it’s linked to depression, anger, and social isolation. People may also drink more because alcohol calms the overactivity.
A Look at Firefighter Steven’s Brain
At age 32, Steven was a firefighter who was suffering from depression, brain fog, and symptoms of unrelenting trauma. During his evaluation, Steven asked, “How can I deal with the trauma? I wish I could forget what my eyes have seen, from children being burned to losing whole families in car crashes and fires.”


Steven’s brain scan showed that his emotional brain—the limbic system—was working way too hard, plus he also had evidence of toxic exposure, likely from breathing carbon monoxide and the poisonous chemicals released from burning furniture. These biological problems in his brain were the root cause of the mental and cognitive issues that plagued him.
Why Firefighters Don’t Seek Help
Studies show that first responders, such as firefighters, are at an elevated risk of trauma, depression, heavy drinking, and suicide. Unfortunately, research shows that they are less likely to seek help because of the stigma associated with having a mental illness, fearing they will be labeled as weak or unfit for duty. Their professions have convinced them that they are supposed to be superheroes, so they just suck it up. Because of this, they continue to suffer in silence.
How a Brain-Based Approach to Treatment Changes Everything
Brain imaging shows that psychiatric issues have a biological basis. In Steven’s case, seeing his scan helped him understand that his “mental health” problems were really “brain health” problems related to toxic exposure and trauma. Rather than thinking his issues were due to some character flaw or weakness, he now viewed them as medical, not moral. This motivated him to get serious about improving his brain health. Within 6 months of following a program designed to optimize his brain, help him deal with trauma, and enhance his body’s ability to flush out toxins, he felt much better and his brain was healthier.
There is no need to suffer in silence. At Amen Clinics, we have helped hundreds of firefighters and other first responders overcome the psychiatric symptoms associated with an unhealthy brain. Whether you’re experiencing depression, anxiety, brain fog, or other symptoms, we offer brain-based treatment programs that use the least toxic, most effective solutions tailored to your needs.
Call 888-288-9834 to speak with a specialist today or schedule a visit online.
At Amen Clinics, we understand that “mental health” is really “brain health,” and for your brain to be healthy, you need a healthy body. If your brain is not healthy, then no matter what medications you take, you will not get better to the greatest degree possible. It’s basically like putting jet fuel in a broken-down car. It just doesn’t work.
What I like about the case study I am going to detail for you here is how beautifully it describes the importance of looking at underlying factors rather than just treating symptoms.
Jake: The Refrigerator Raider
This is the story of Jake and his wife Gen (names have been changed).
For 8 months, Gen had been suffering almost nightly with an eerily similar pattern. Between 2-4 a.m., Gen would feel Jake get up and go out to the kitchen where he would rummage through the pantry and refrigerator, eat messily like he was in a hot dog eating competition, then head back to the bedroom, leaving a trail of food and crumbs like Hansel and Gretel all the way back into their bed.
She would also notice a glazed look in his eyes, as if he was not all there, and was afraid to wake him out of it.
As understanding as she was, she was just not the kind of woman who fancied waking up next to a snoring partner in a bed full of crumbs with the first chore of the day having to be cleaning up after him.
Between his incessant snoring, messy night-time eating habits, and other issues, Gen was at her wit’s end and needed solutions. Fast. So, she recorded his bizarre sleeping behaviors on video, which is a great idea for a partner to do, and convinced him to come to see me.
In discussing his history, I learned that Jake was a 39-year-old veteran (served in Iraq and Afghanistan), with a medical history of obesity (body mass index 36), post-traumatic stress disorder (PTSD), alcohol abuse (in the past), vitamin D deficiency, hypothyroidism, and chronic pain.
The sleep complaints included snoring, nightly sleep-eating behaviors, excessive daytime sleepiness (Epworth Sleepiness Scale of 16), fatigue, non-refreshing sleep, and weight gain of over 40 pounds in the last 8 months.
Now it was time for me to solve the case.
Decoding Multiple Health Issues
As clinicians, it is very important that we understand how different health issues impact one another. This was very true in Jake’s case.
Jake was obese, which is a risk factor for obstructive sleep apnea (OSA). In this condition, the airway collapses and the tongue periodically falls back in the throat during sleep, closing off the airway and resulting in symptoms like snoring, tiredness, sleepiness, depression, lack of motivation, and concentration problems. It also puts a lot of strain on the heart, resulting in less blood flow to the brain and an increased risk of dementia, anxiety, heart attacks, high blood pressure, strokes, and sudden death.
Several times during the night, the brain can wake up (arousals) in order to trigger the muscles to breathe and get oxygen to the brain. Hence, sleep apnea also leads to excessive sleepiness, which can result in workplace and traffic accidents. It is estimated that 6,400 fatal accidents each year in the U.S. are attributed to sleep apnea. Frost & Sullivan calculated that the annual economic burden of undiagnosed sleep apnea among U.S. adults is approximately $149.6 billion. The estimated costs include $86.9 billion in lost productivity, $26.2 billion in motor vehicle accidents, and $6.5 billion in workplace accidents.
Jake’s sleep-related eating disorder is a form of parasomnia—any abnormal behaviors that occur during sleep—and involves binge eating during the sleep period. Typically, it is associated with minimal recollection or conscious control as well as weight gain. In some instances, sleep eating episodes may be caused by arousals related to untreated OSA that occur during sleep.
Other types of parasomnias—such as sleep talking, sleepwalking, or confusional arousals—can be a clue not just to sleep apnea, but also to chronic sleep deprivation. In sleep deprivation, we are concerned not only with the total amount of sleep somebody gets, but also the quality of that sleep. If you get 8 hours of sleep a night, but you have sleep apnea and are waking up tired, it is not adequate sleep. In fact, it is terrible sleep because every minute you are asleep with untreated OSA, your brain is suffocating. In some cases, parasomnias may be the result of something more serious, such as a seizure disorder.
We know that parasomnias like sleep eating disorder tend to occur most commonly in the transitional period between sleep and wakefulness.
Additionally, there was Jake’s PTSD to consider. When the nervous system is on high alert as it is in syndromes like PTSD, a person may tend to breathe heavily and blow off a lot of carbon dioxide. The brain can detect a drop in carbon dioxide and even trigger the muscles to stop breathing periodically to get the levels of carbon dioxide up to normal levels.
This is called central sleep apnea and is yet another way that the brain can be deprived of oxygen. The brain can then wake up, slip into the transitional zone between sleep and wakefulness, and trigger another parasomnia episode like sleepwalking and sleep eating.
Studies also suggest PTSD may be a risk factor for sleep disruption and sleep apnea, and treatment of OSA improves PTSD symptoms.
In Jake’s case, I had to look into the association between sleep apnea, PTSD, weight gain, sleepwalking, and sleep eating and how they perpetuate an unhealthy sleep cycle. In addition, a clinician must consider other factors, such as:
- Sleep deprivation (which can make your brain go into deeper stages of sleep to make up for lost sleep and can trigger arousals from deep sleep and parasomnias)
- Primary insomnia
- Medications (those that can affect REM or NREM sleep or cause sleep disruption independently or by worsening other sleep fragmentation disorders
- Co-morbid illnesses (such as low vitamin D, chronic pain, and other illnesses that can disrupt sleep)
To best serve our patients, we must be aware of how all these different factors may come together.
Pinpointing Jake’s Diagnosis
Let’s go back to Jake, whose main concern was his sleep-eating behaviors, which resulted in a weight gain of over 40 pounds. Gen’s main concerns were his snoring and sleep eating (which were destroying her sleep and ruining her mood), as well as his sleepwalking (which made her worry that Jake might hurt himself).
On reviewing details of Jake’s mental health history, as well as his sleep history, I discussed how sleep deprivation can worsen sleep disordered breathing (sleep apnea) and likewise, how sleep disordered breathing can lead to disrupted sleep, which can then perpetuate parasomnias like sleepwalking and sleep eating. Adding in Jake’s hyper-arousal (PTSD), which has been linked to an increased risk of sleep disordered breathing, compounded the sleep disruptions and consequent parasomnia (sleep eating), which in turn caused weight gain and worsened sleep disordered breathing.
Thus, my running hypothesis was that sleep-eating behaviors could be a secondary disorder of arousal due to severe sleep apnea.
To better understand Jake’s sleep patterns, I ordered a nocturnal polysomnography, a sleep study that involves the following:
- Sensors on the head to detect brain waves
- Belts on the chest and belly to detect breathing patterns
- A sensor to detect oxygen levels of the blood
- A microphone to detect snoring
- Sensors on the limbs to detect movements during sleep
- A sensor to detect body positioning
- Infrared video monitoring of the room
- A sensor near the nose to detect the temperature and pressure of the air going in and out of the nose.
Jake’s study demonstrated severe sleep apnea with an overall AHI (Apnea Hypopnea Index) of 108.3 events per hour. This means that Jake stopped breathing over 108 times an hour.
This is dangerous and requires immediate treatment because of the risks of untreated sleep apnea, as discussed previously.
I put Jake through another sleep test, in which different levels of CPAP (continuous positive airway pressure) are tried. Here, they monitor how many times the person stops breathing, as well as what pressures work best and are best tolerated. This device works because the pressure of the air delivered from the machine via tubing and a mask can keep the airway open and prevent its collapse.
The study concluded that pressures of between 8-14 cmH2O worked best to minimize the pauses in breathing. I hypothesized that if the sleep apnea was controlled adequately, there would be fewer arousals from sleep into sleepwalking and sleep eating. This would result in weight loss, which would further improve the sleep apnea. Controlling the sleep apnea would also improve his symptoms of PTSD.
I followed Jake for several months, making adjustments to his CPAP machine, getting downloads from the machine to make sure it was doing what it was supposed to be doing. In addition, I treated his PTSD independently and utilized a whole-brain approach to his health that included exercise, nutrition, targeted supplements, and cognitive behavioral therapy for insomnia.
Over time, he regained his energy, his symptoms of depression subsided, his concentration improved, his weight dropped, and his overall quality of life improved. His snoring was eliminated, and the nightly sleep-eating resolved for the most part, much to the delight of Gen, his patient wife.
Jake had his life back and had the tools he needed to be the father, husband, employee, family member, and friend that he wanted to be.
About the Author: Shane Creado, MD, Amen Clinics Chicago
Dr. Shane Creado is a board-certified psychiatrist and sleep medicine physician. He is also a sports psychiatrist and is on the Board of Directors of the International Society for Sports Psychiatry, as its Chairman of Memberships. Additionally, he has clinical experience with the veteran population, college mental health, exercise prescription and mental health, co-morbid psychiatric and sleep problems, CBT-Insomnia, alcohol recovery groups, MBSR (Mindfulness-Based Stress Reduction), administrative psychiatry, health care policy, cultural psychiatry, couples therapy, and regressive hypnosis. He uses the skills he acquired in these disciplines to holistically apply evidence-based medicine in the service of his patients. In his spare time, he likes to travel, write, act on stage, and play racquet sports.
By Rishi Sood, MD, ABPN
Imagine waking up every morning feeling sad, exhausted and hopeless. You go to the doctor and after a brief visit, you are prescribed a medication that is intended to increase serotonin (the “happy” chemical). After 4 to 6 weeks you are told that you should see improvement, but your symptoms get worse. You return to the doctor and are told to discontinue the treatment and over the course of several years go through several medication trials and all sorts of psychotherapy, which do not help. More aggressive approaches are tried. However, Transcranial Magnetic Stimulation, ECT, and Ketamine (used in treatment-resistant cases) fail to provide relief. Over this time period, your marriage ends, you become unemployed and the only purpose to continue living is to see your children grow. Unfortunately, this had been Kevin’s journey when he arrived at the Amen Clinics New York in September of 2017.
When I met Kevin for an initial consultation, he shared that we were his last hope. We agreed that we needed to take a deeper look to determine what we were missing. We began by taking a detailed childhood developmental history.
It was evident that Kevin was exposed to early childhood trauma. His earliest memories were of his parents arguing with the quarrels turning violent when his father would drink alcohol. His older sister would intervene, while Kevin would avoid conflict altogether and use video games to escape reality. Kevin was described by peers and teachers as a shy, introverted, well-behaved boy, but what no one could see is how much Kevin struggled with focus. When teachers would lecture, he would zone out or, as he described it “my brain would shut down.” Completing homework took more than four hours when it should have taken one to two hours to complete. Kevin was able to get “average” grades but often felt inferior as his parents would compare him to Asian peers who were excelling in their tight-knit community. His mother would tell him to work harder and berate him for being lazy. During his adolescence, Kevin turned to marijuana to numb his feelings of inadequacy and decrease overall stress.
Hearing this, I began to think of Kevin’s poor brain. I had an idea of what could be going on but needed to actually look at his brain to really have a clear picture.
When we scanned his brain, several subcortical structures were much more active as compared to healthy controls for his age group. A “diamond pattern” was seen in both resting and concentration states. We often see this pattern in individuals who have experienced emotional trauma and suffer from Post-Traumatic Stress Disorder (PTSD). It was as if Kevin’s brain was on high alert ready to defend against any threat when there was no threat.

It was also evident that Kevin had frontal lobe dysfunction which worsened when he concentrated. The frontal lobe is the “Executive Center” of our brain and governs concentration and short-term memory. This explained Kevin’s struggles in school and in his marriage where he reported: “not being able to keep up with daily responsibilities which led to severe disaccord between me and my ex-wife.”

In order to effectively help Kevin, it was imperative that both systems (frontal lobe and subcortical) needed to be targeted. Upon review of prior treatment plans, both systems were in fact targeted but never together.
The first phase of treatment involved quieting the subcortical circuitry without causing further frontal lobe dysfunction. Our research has shown that a particular class of medications (SNRI-Selective Serotonin Norepinephrine Inhibitors) can drastically reduce depressive symptoms when dealing with these specific brain patterns. We started Venlafaxine (SNRI) and within six weeks Kevin began to report less obsessional thinking, and agitation and was no longer in a constant “fight or flight state.”
To help further decrease the high activity in the emotional trauma circuitry, Kevin completed several sessions of Eye Movement Desensitization Processing (EMDR). During the EMDR therapy, Kevin attended to emotionally disturbing material (i.e. witnessing his father physically abusing his mother). The EMDR therapy facilitated the accessing of his traumatic memory network so that information processing was enhanced, with new associations forged between the traumatic memory and more adaptive memories or information. Kevin reported that the memories “no longer controlled me, it was as if I was free from the past.”

Despite his improvement, Kevin continued to report struggling with attention which made sense as we still had work to do on his frontal lobe. Kevin and I agreed to take more of a natural approach, before adding more medication. We started Omega 3 Power and L-Tyrosine to increase dopamine levels. Within two weeks Kevin reported improved concentration and within three months read a novel cover to cover for the first time in his life.

Kevin understood that taking the medication and supplementation provided the scaffolding to aid in recovery. To take his brain health to the next level he would need to do more. Now that the depression had lifted, he was motivated. Kevin began to exercise (High-Intensity Interval Training 3 times per week) and eliminated processed sugar from his diet. This further increased energy levels and enhanced sleep.
In just 6 months, Kevin’s condition had dramatically improved and he reported having a “new lease on life.”
As I reflect on Kevin’s case, I cannot help but wonder, “What would have happened to Kevin had we not looked at his brain?” I do not believe we would have been able to help Kevin. This case highlights how critical it is to understand the interplay of brain systems and how optimization in a specific sequence can lead to dramatic improvement.
We continue in our quest in helping others, with the hope that one day everyone will have the opportunity that Kevin had. When Kevin changed his brain by doing the things we recommended, he changed his life.
About the Author: Rishi Sood, MD, ABPN
Dr. Sood values working with adults and children across all age ranges. He is experienced in mood and anxiety disorders, addiction, ADD/ADHD, impulsive/disruptive behavior disorders, Autism Spectrum, psychotic disorders, OCD, and PTSD. He uses dynamic as well as cognitive-behavioral therapy, interpersonal psychotherapy, family psychotherapy and works to integrate pharmacotherapy and alternative therapies to optimize brain health and function. Behavioral change is a process and Dr. Sood incorporates a motivational interviewing approach into evaluations to support the client and meet them where they are at, offering client-centered care. He firmly believes that clients do well with continued support in their journey toward optimal brain health.
In the field of psychiatry, there seems to be a new “diagnosis du jour.” A rising number of people are being diagnosed with bipolar disorder, also known as bipolar spectrum disorder (BSD). Up until the year 2000, bipolar disorder (formerly referred to as manic-depressive illness) was diagnosed at a rate that hovered around 0.4%-1.6%. By the 2000s, that number jumped to 5%-7%. These days, it’s reached fad status.
Many people walk into a psychiatrist’s office and say, “I’m bipolar” or they’ve been diagnosed with the condition. But there’s a problem—many of them don’t actually have the disorder, which is associated with dramatic swings in moods and energy levels that repeat in a cyclical pattern. A 2008 study found that 57% of people diagnosed with bipolar disorder had been misdiagnosed.
That’s what happened to Jessica. She was dealing with severe moodiness and after a 10-minute visit with her primary care physician, was diagnosed with the condition and given a prescription for mood stabilizers. But the medication wasn’t working. A functional brain scan using SPECT technology showed why. Jessica was suffering from the lasting effects of concussions she suffered from multiple bicycle accidents. She didn’t have bipolar disorder; she had a traumatic brain injury (TBI) that needed healing. With the right treatment plan, her moods improved, and she started feeling like her old self again.
7 Conditions Commonly Misdiagnosed as Bipolar Disorder
- TBI: Head injuries can cause symptoms of depression, irritability, fatigue, and changes in sleep patterns—all things that can also be seen in people with BSD.
- Depression: Persistent sadness, loss of interest in usually pleasurable activities, and decreased energy are seen in both depression and in the depressive episodes of BSD. Because of this, it’s common for depression and bipolar disorder to be mistaken for the other.
- ADD/ADHD: The manic episodes of bipolar disorder and ADD/ADHD have many common symptoms, including impulsivity, racing thoughts, restlessness, trouble concentrating, and irritability.
- Post-traumatic stress disorder (PTSD):The feelings of hypervigilance, irritability, and sleep issues found in PTSD can mimic the symptoms of mania in bipolar disorder, leading to misdiagnosis.
- Anxiety: The racing thoughts, heart palpitations, and trouble sleeping that can come with anxiety are also signs of manic episodes of BSD.
- Schizophrenia:About half of all people with bipolar disorder experience psychotic symptoms, such as hallucinations or delusions, which are hallmarks of schizophrenia. For this reason and because bipolar disorder is more common in the U.S.—about 2.8% of adults are affected by bipolar disorder compared with just 1% who have schizophrenia—people with schizophrenia are more likely to be misdiagnosed.
- Borderline personality disorder (BPD): Common traits seen in both BPD and bipolar disorder include unstable moods, impulsivity, irritability, and relationship troubles. This leads to an overdiagnosis of bipolar disorder. Research shows that 40% of people with BPD had previously been misdiagnosed with bipolar disorder.
The Consequences of a Bipolar Disorder Misdiagnosis
Being mistakenly diagnosed with bipolar disorder is problematic because the treatments for it typically won’t work to heal other conditions and could make them worse. Some people who have been misdiagnosed with bipolar disorder spend years going from one mood-stabilizing medication to another without relief. This can increase the risk of alcohol and drug abuse as a way to self-medicate and also raises the risk of suicidal thoughts and behavior.
The Path to an Accurate Diagnosis
Because there are so many overlapping symptoms associated with bipolar disorder and other conditions, simply assessing symptom clusters isn’t enough to make an accurate diagnosis. Functional brain imaging studies using a technology called SPECT can help accurately distinguish brain patterns associated with bipolar disorder, ADD/ADHD, depression, TBI, and other conditions.
At Amen Clinics, we use leading-edge brain imaging technology called SPECT as part of an overall evaluation to accurately diagnose and treat mental health conditions, such as bipolar disorder. If you or a loved one has been diagnosed with bipolar disorder and treatment isn’t working, it’s important to understand if you have been misdiagnosed. Getting an accurate diagnosis is critical to finding the relief you want from your symptoms, so don’t hesitate to schedule a visit or call to speak to a specialist at 888-288-9834.
If you’ve lived through a traumatic event, it’s natural to think that as time passes, you’ll get over it and move on with your life. But that doesn’t always happen. Symptoms of post-traumatic stress disorder (PTSD) can occur right after a terrible event, or they can emerge weeks, months, or even years after a traumatic incident. PTSD can also be chronic after years of abuse or growing up in an unpredictable and stressful home, such as with an alcoholic or drug-abusing parent. Persistent early childhood trauma can set kids up for PTSD later in life.
Because PTSD symptoms may not emerge immediately, you may not connect your distressing symptoms with the trauma you experienced.
5 Types of Symptoms that May Indicate You’re Suffering from PTSD
1. Memory Issues
PTSD can impact your memories in a number of ways. You might experience recurrent upsetting thoughts or dreams of a past traumatic event. Flashbacks can pop up at any time—even when you’re in a familiar place—and make you feel like you’re experiencing the trauma all over again. You may find that you’re unable to stop thinking about the event, and distressing thoughts loop incessantly in your head. In other cases, you may have lapses in your memory regarding certain aspects of a traumatic event.
2. Increased Anxiety
It’s common for people with PTSD to feel constant anxiety or to experience panic attacks. You may be easily startled or feel like you’re always on guard, expecting something bad to happen at any moment. Some people with PTSD say they feel “jumpy” or “jittery.”
3. Avoidance
If you purposely steer clear of anything—people, places, or things—that reminds you of the traumatic event, it could be a sign of PTSD. You may avoid talking about the event and refuse to share your feelings about what happened.
4. Mood Changes
If you experience a persistent sense of hopelessness, feel emotionally numb, or lose interest in things you used to enjoy, it could be connected to the trauma. You may not make that connection though and might mistake these symptoms as depression rather than PTSD. You may also feel shrouded in a strong sense of guilt and shame.
5. Behavioral Issues
Having PTSD can change the way you behave. You may isolate yourself from your friends and family, which robs you of an important support network and compounds your other symptoms. Increased irritability can cause you to lash out at others in anger. Or you may engage in self-destructive behavior, such as abusing drugs or alcohol.
If you’ve experienced any of these symptoms, it’s a good idea to seek help. However, because many of these symptoms are also associated with other conditions, such as anxiety, depression, or even traumatic brain injury (TBI), it can make it more challenging to diagnose PTSD based on symptoms alone. If PTSD is misdiagnosed, you may be given medication or other treatments that not only don’t help, but that also make your symptoms worse.
Getting an accurate diagnosis is critical to healing from PTSD. Brain imaging can help. Brain SPECT studies can identify patterns associated with PTSD so you can get the right treatment plan to help you begin the healing process.
SPECT Imaging of PTSD Before & After Treatment
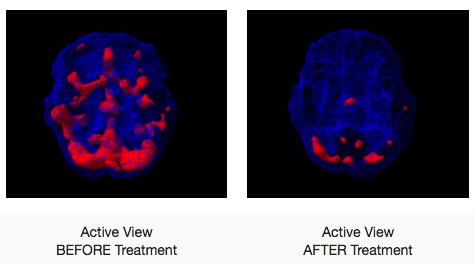
If you or a loved one has experienced a traumatic event and is experiencing symptoms of PTSD, it’s important to seek help. At Amen Clinics, we perform brain SPECT scans as part of a complete evaluation to diagnose and treat PTSD with the least toxic, most effective solutions.
Don’t let PTSD steal your life. Call one of our brain health advisors at 888-288-9834 to see how Amen Clinics can help or schedule a visit online.
EMDR (eye movement desensitization and reprocessing) is a special psychotherapeutic technique that can be a very powerful treatment for people who have been emotionally traumatized. EMDR therapy uses eye movements or other alternate hemisphere stimulation to remove the emotional charges of traumatic memories.
As part of EMDR therapy sessions, a therapist may direct you to hold specific memories in mind while tracking the therapist’s hand as it moves back and forth across your field of vision. Diverting your attention in this way while you recall a traumatic event has been found to minimize the emotional response connected to the memory. Researchers believe the therapy activates mechanisms in the brain that help you process the memory and distressing emotions.
Processing Traumatic Memories in the Brain
The brain is naturally wired to help us recover from traumatic events and distressing memories. The healing process involves communication between a variety of brain regions, such as the hippocampus (memory-making center), amygdala (fear center), and prefrontal cortex (behavior center). In some people, however, events can be so traumatic it disrupts the normal flow of neural communication and memories get stuck, making you can feel like you are frozen in time. EMDR helps you get unstuck by restoring the communication process.
What Research Shows About EMDR
Numerous studies show that EMDR therapy offers benefits for emotional trauma and PTSD that typically take years to achieve in psychotherapy alone. A 2014 review of the existing research indicates that 24 randomized controlled studies point to benefits from EMDR treatment for emotional trauma and adverse life events. This review also showed that in some studies, 84% to 90% of people who have experienced a single trauma found relief from PTSD symptoms after just 3 EMDR sessions that lasted 90 minutes each.
In a controlled study by Kaiser Permanente, 67 individuals who had experienced trauma were assigned either to standard care treatment or EMDR. Compared to standard care, the EMDR group showed significantly more improvement on measures of anxiety, depression, and PTSD. In a subsequent study from the same team at Kaiser Permanente, follow-ups on the original study participants at 3 months and 6 months showed that improvements from EMDR had been maintained. The authors concluded that long-lasting benefits can be achieved with relatively few EMDR sessions.
Based on this growing body of research, the American Psychiatric Association and the Department of Veterans’ Affairs have recognized EMDR therapy as an effective treatment for PTSD. A growing body of research on EMDR therapy shows promising results in its effectiveness for other conditions, such as depression, addictions, and more.
Who Can Benefit from EMDR?
EMDR is primarily used to treat people suffering from emotional trauma, but it may also be beneficial for people struggling with other problems. According to the EMDR International Association, practitioners currently use EMDR therapy to address a wide array of issues, including but not limited to:
- PTSD
- Depression
- Bipolar disorder
- Anxiety
- Panic attacks
- Phobias
- Substance abuse
- Eating disorders
- Dissociative disorders
- Personality disorders
- Grief
What’s Involved in EMDR Therapy?
EMDR therapy involves 8 phases that incorporate a variety of elements. It includes looking at past memories, current triggers, and skills and behaviors that can help you in the future.
Phase 1: History and Treatment Planning
A therapist will review your history, identify specific memories to target, and create a treatment plan.
Phase 2: Preparation
The therapist will share several techniques to help you cope with any emotional distress that may arise during treatment.
Phases 3: Assessment
During this portion of the treatment, you will be directed to identify 3 things associated with the targeted memory to be processed:
- a visual image related to the memory
- a negative belief about yourself
- any physical bodily sensations associated with the memory
Phase 4: Desensitization
As you hold these things in mind, the EMDR processing begins. After the therapist performs the hand movements or other stimulation, you will be asked to let your mind go blank. Then you may either return to continue processing that same memory or move on to process other memories.
Phase 5: Installation
Here you replace the negative belief you had about yourself with a positive belief. For example, a victim of assault may go from believing “I am powerless” to believing “I am in control.”
Phase 6: Body Scan
During this phase, your therapist will work with you to resolve any remaining physical tension or bodily sensations related to the memory.
Phase 7: Closure
The therapist will ensure that at the end of each session, you feel better than when it started. Your therapist will also provide you with strategies to help you handle any distressing emotions that come up in between sessions and will ask you to maintain a journal where you write down any issues that arise.
Phase 8: Reevaluation
At each session, you and your therapist will assess your progress so far and adjust your treatment plan as needed.
Steven’s EMDR Story
To help you understand how EMDR can work for emotional trauma like PTSD, take a look at Steven’s story.
Steven, a 33-year-old bicycle repair mechanic working in Santa Monica, California, took an early lunch on a summer day in 2003 and walked to the local farmer’s market. Within minutes, disaster struck when an 87-year-old man lost control of his car and barreled through the throngs of people at the market. The car was headed straight for Steven, who later said, “I thought he was going to run over my legs…I thought I would lose my legs.”
At the last possible moment, Steven was able to jump out of the way, but 10 people were killed and more than 50 were injured. Traumatized, Steven went back to work. But for months, he couldn’t sleep, and he shook constantly. As in the case of most people who develop PTSD, the Santa Monica farmer’s market disaster was not Steven’s only trauma. He grew up in a severely abusive alcoholic home and also faced death as a tank commander during the Gulf War.
Steven decided to undergo an evaluation and EMDR therapy as a component of his treatment. As part of his assessment, Steven underwent 3 brain scans using brain SPECT imaging technology—before treatment, during his first EMDR session, and after 8 hours of EDMR treatments.
Initially, his brain scan showed a diamond pattern that is often seen in PTSD, with an overactive limbic area, basal ganglia, and anterior cingulate. Then with the help of a trained EMDR therapist, Steven began clearing out the traumas—one by one. His brain actually showed benefit during the first treatment and was markedly improved after only 8 hours of treatment. Steven’s shaking had subsided, and he felt significantly better. With EMDR, Steven was able to change his brain and change his life for the better.
PTSD, emotional trauma, and other mental health issues can’t wait. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, clinical evaluations, and therapy for adults, teens, children, and couples. Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here.
Post-traumatic stress disorder (PTSD) gets a lot of press, especially regarding military veterans who return from combat. For example, it’s estimated that 11-20% of veterans who served in the recent wars in Iraq and Afghanistan have PTSD in a given year.
However, you don’t have to see combat in the military to be vulnerable to PTSD, a potentially debilitating condition that can lead to intrusive thoughts and flashbacks, avoidance of reminders of the traumatic event, feelings of guilt, a sense of being on edge at all times, being easily startled, anxiety or depression, problems sleeping, as well as other symptoms.
You may be surprised to discover that PTSD can affect anyone—any ethnicity, nationality, or age—although women are 2-3 times more likely to develop the condition than men. Approximately 3.5% of adults in the U.S. are affected by the condition, and about 7-8 people out of 100 will have PTSD in their lifetime.
What’s even more surprising is that in some cases, you don’t even have to be involved first-hand in a traumatic event. Simply hearing about a traumatic event or repetitive viewing of violent news stories on television can increase the risk of PTSD.
10 Types of Traumatic Events That Can Lead to PTSD
- Military combat
- Rape or other physical assault
- Childhood abuse
- Natural disasters
- Automobile accidents
- Sudden death of a loved one
- Seeing someone get seriously hurt or killed
- Being held at gunpoint
- Terrorist attack
- Mass shooting
Not everybody who is exposed to a traumatic event will develop PTSD. Certain things can make you more vulnerable to the condition, including having little or no social support in the wake of a traumatic event, as well as coping with additional stresses due to injuries, the death of a loved one, or the loss of your home.
What the Media Gets Wrong About PTSD
Most media articles talk about PTSD as a psychological problem, but that isn’t accurate. Although it does cause psychological consequences, PTSD is, in fact, a brain disorder. Brain imaging studies using a technology called SPECT show PTSD is associated with changes in the brain. Without brain imaging, PTSD is often misdiagnosed because symptoms overlap with other conditions, such as traumatic brain injury. Research shows that brain scans help differentiate PTSD from TBI to help you get an accurate diagnosis and more effective treatment.
If you or a loved one has experienced a traumatic event and is experiencing symptoms of PTSD, it’s important to seek help. At Amen Clinics, we perform brain scans using a technology called SPECT as part of a complete evaluation to diagnose and treat PTSD with the least toxic, most effective solutions.
Don’t let PTSD steal your life. Call one of our brain health advisors at 888-288-9834 to see how Amen Clinics can help you or schedule a visit online.
Veterans with PTSD are over four times more likely to have suicidal thoughts as those who don’t suffer from the condition. And those who have suffered multiple traumatic brain injuries are twice as likely to consider suicide compared with those who have experienced a single TBI or no brain trauma. These conditions also increase their risk of homelessness, incarceration, and substance abuse.
In 2008 Capt. Patrick Caffrey was deployed in Afghanistan with the Second Battalion, Seventh Marines (2/7) Combat Engineer Platoon. The combat engineer officer was tasked with an intense mission—detect and clear mines and Improvised Explosive Devices (IEDs) from roads so the infantry and convoys could pass through safely. Helping protect Caffrey and his platoon were new, specially armored vehicles. “They could take an enormous blast, and you’d be able to walk away unscathed—or so we thought,” he says.
While in Afghanistan, Caffrey experienced three blasts and sustained three concussions, but he walked away each time. He was no stranger to concussions; he had already had five or six of them from playing sports and other injuries. But he felt okay, so he thought everything was fine.
It wasn’t.
Over time, Caffrey’s personality began to change. “I was more irritable than ever, I had intense headaches, trouble focusing and concentrating (particularly listening to what people were saying), trouble with memory, and an inability to sleep,” he says. “I was rude and nasty to people and the worst part was that I didn’t really know just how much I had changed.”
When he sought help, the diagnosis wasn’t clear-cut. His symptoms pointed to two possibilities: posttraumatic stress disorder (PTSD) or traumatic brain injury (TBI).
The Problem with Overlapping Symptoms
Caffrey isn’t alone. Since 2000, more than 500,000 veterans and active military personnel have been diagnosed with PTSD, TBI, or both. Unfortunately, these debilitating brain issues can be difficult to distinguish because they share many of the same symptoms, including:
- Increased or excessive anxiety
- Feeling emotionally numb
- Problems with sleep
- Anger and irritability
- Depressive symptoms
- Social isolation
In the field of psychiatry, diagnoses are typically made by looking for symptom clusters. For this reason, PTSD and TBI can be misdiagnosed, which can have dire consequences.
The Consequences of Guesswork
Although the symptoms are similar, the treatments for PTSD and TBI are vastly different. More importantly, the treatments for PTSD can be harmful to those with TBI and, likewise, remedies for TBI could be detrimental to those with PTSD.
Misdiagnoses and treatment failures mean our nation’s veterans can spend years trying to get relief for their symptoms. In the meantime, haunting memories and debilitating symptoms can hold them captive and get in the way of work, relationships, family life, and life itself.
Although our society has engineered advanced robotics that is helping troops heal from the physical damages of war, we as a nation are failing our veterans on the mental health front.
The Veterans Administration, like most in the field of psychiatry, continues to diagnose and treat people based on symptom clusters, the same way mental health professionals have been practicing for over 100 years. In terms of treatment, they are basically throwing darts in the dark at the problem.
The current administration has established a task force on veteran suicide that will research ways to prevent and treat the problem. This sounds promising, but if we continue to throw money at an outdated treatment model, we will lose the battle.
We can do better.
Brain Imaging Offers a New Model
“The traditional model isn’t working. The system that is supposed to be supporting our veterans is failing them,” according to Dr. Jomar Suarez at Amen Clinics Northern California, who is involved in research that is looking at how brain imaging technology called SPECT can help reverse these devastating trends.
A study led by Amen Clinics that appeared in 2015 issue of PLOS One found that SPECT brain imaging technology, which measures blood flow and activity in the brain, could effectively distinguish PTSD from TBI with a 94% accuracy rate. By comparison, MRI and CT scans often show “normal” results, which makes veterans think they are imagining their symptoms.
According to the SPECT research study, which was ranked #19 on Discover Magazine’s Top 100 discoveries of the year in 2015, patients with TBI show decreased activity in certain areas of the brain. In PTSD patients, however, there is increased activity in some brain regions.
In an effort to get an accurate diagnosis and the right treatment, Caffrey decided to undergo the brain imaging test. His SPECT brain scan revealed damage to his right temporal lobe, which explained his behavioral and cognitive changes, headaches, decrease in ability to focus and concentrate, and memory issues. There was also too much activity in some regions. The SPECT findings, combined with his personal history and symptoms, indicated that he had both PTSD and TBI.
“Boy, did I underestimate the value of actually looking at the brain when you have a brain problem!” he said.
Capt. Caffrey’s Brain Scans
TBI: damage to right temporal lobe and decreased activity.

PTSD: Increased activity.

Hope for Suicide Prevention
Additional research is currently underway to investigate if adding SPECT brain imaging to the traditional model practiced at the VA could improve diagnostic accuracy and treatment effectiveness within the veteran population for other conditions, such as depression, as well as suicide prevention.
Preliminary data from a 2019 SPECT research project being undertaken by Amen Clinics and No Vet Alone on a small group of veterans showed promising results. Among the participants who were taking medication and still experiencing disabling symptoms, “75% had SPECT scans that suggested a different medication might be more effective,” says Suarez. “This suggests that with SPECT, we can avoid a lot of the trial-and-error involved in the traditional model and target and treat brain imbalances more effectively.”
This most recent project, which Suarez hopes to expand to a larger research study, showed other potential benefits of brain imaging. For example, among the veterans who were opposed to taking medications due to past treatment failure, seeing their brain scans opened their mind to taking medication targeted to their needs.
In addition, in 100% of the veterans involved, SPECT brain scans suggested additional therapies beyond medications that might help, including hyperbaric oxygen therapy, neuromodulation, EMDR, nutritional supplements, and more.
Suarez says one of the overarching goals of the project is to identify brain imaging biomarkers that may help predict veterans who are suicidal and ultimately prevent suicide.
A Path to More Effective Treatment
In Caffrey’s case, the brain scan helped create a rehabilitation program that was targeted to treat both conditions. “I felt a dramatic difference right away,” he says. “I felt more mentally sharp and focused than ever.” Caffrey has continued to improve and says, “Ultimately, the scan was my gateway tool to a set of brain healthy strategies that I still use to have a better brain and a better life.”
Capt. Caffrey’s brain scan was performed at Amen Clinics, which has the world’s largest database of functional brain scans and is where the 2015 PLOS One brain imaging study was conducted. Amen Clinics has treated hundreds of people, including veterans, with TBI, PTSD, and other co-existing conditions and is able to tailor more effective treatment plans based on SPECT brain imaging technology.
If symptoms of PTSD, TBI, or co-existing conditions are impacting your life or you aren’t responding to treatment, call 888-288-9834 to speak to a specialist or schedule a visit online.
According to the National Institutes of Mental Health – 51 percent of the U.S. population will suffer from a mental health issue at some point in their lives. Regrettably, the matter of mental health remains shrouded by misconceptions and harmful stereotypes. Many people with mental health problems feel that the stigma and discrimination they experience from their family, friends, employer, and society itself, makes their symptoms worse and delays the recovery process. Frequently overlooked in the ongoing mental health conversation are pregnant women. How can these women get help for their mental or emotional challenges? The field of perinatal psychiatry is attempting to answer that question.