SPECT Gallery
A Look Inside the Mind with Brain SPECT Imaging
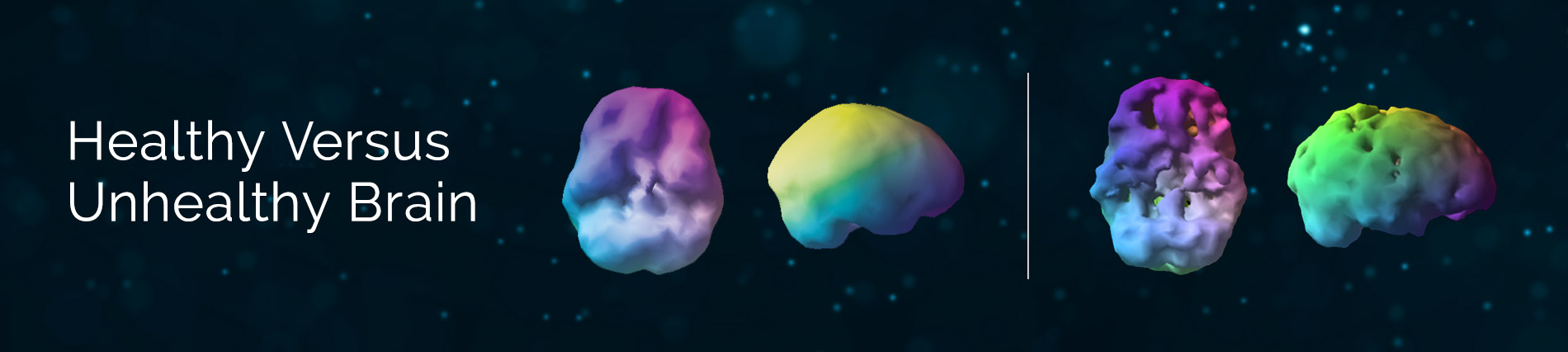
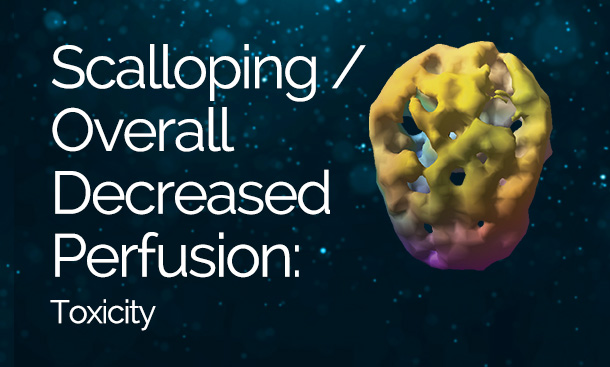
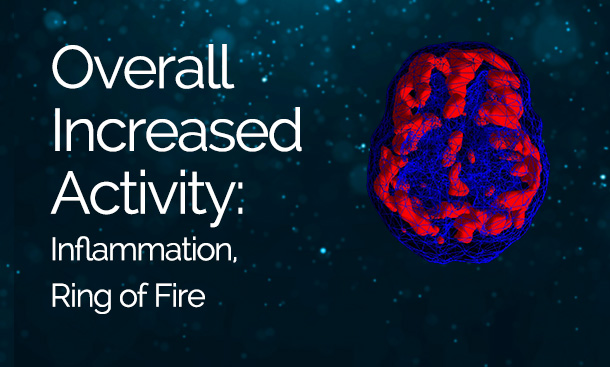
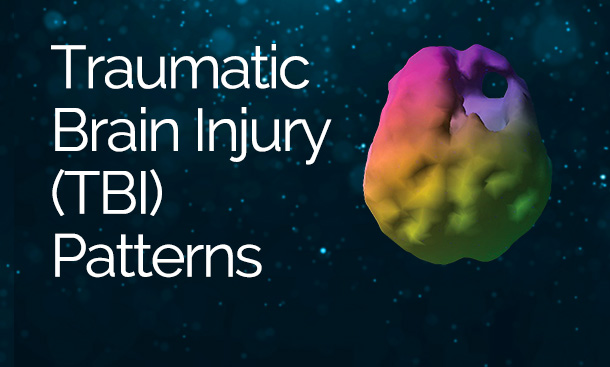
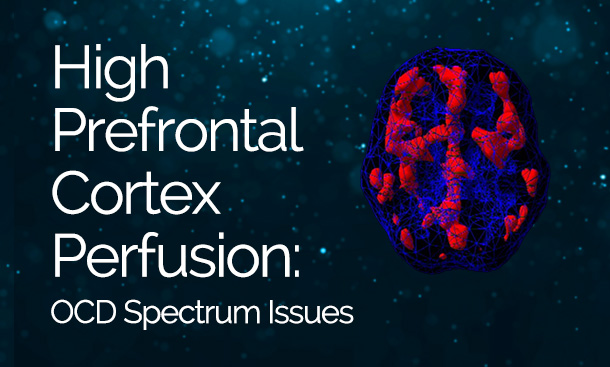
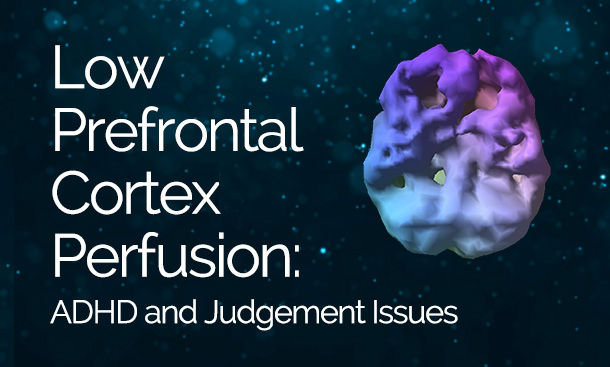
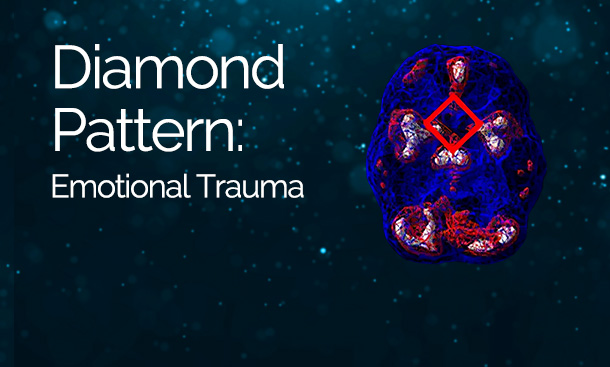
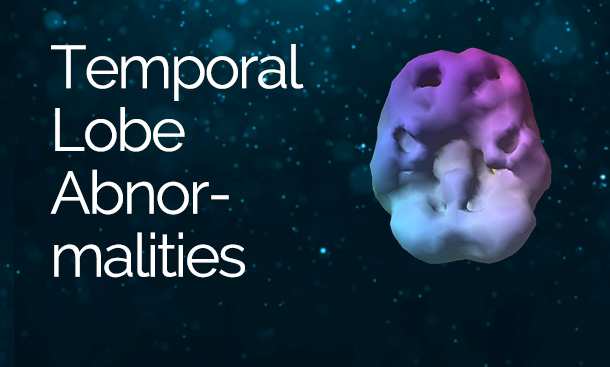
Brain SPECT imaging is a state-of-the-art brain mapping tool that measures blood flow and activity patterns and allows us to see areas of the brain with healthy activity, too little activity, or too much activity. Discover some of the most common brain patterns seen at Amen Clinics.