Some people think that age-related brain changes are an inevitable part of life. But cognitive decline does not need to be part of anyone’s story. There are numerous ways to start protecting your brain health—and these should remain a priority at any age.
Maintaining a healthy brain encompasses more than just avoiding well-known neurodegenerative diseases such as Alzheimer’s and other types of dementia. A healthy brain supports mental health, improves focus and memory, and boosts overall well-being. Simply put, you can’t be healthy if your brain isn’t healthy.
Fortunately, regardless of your age, you can strive for lifelong brain health by taking certain helpful steps. Whether you’re raising small children or have reached your senior years, in this blog, you’ll find age-specific strategies that will help protect the body’s most complex and incredible organ: the brain.
New authoritative textbook—Diagnostic Imaging: Brain, Fifth Edition—establishes that functional neuroimaging tools, including SPECT, can detect telltale patterns of CTE in the brain while the individual is still living.
The possibility of early SPECT detection marks a major shift in how medical experts can evaluate and treat those with CTE.
In this blog, you will learn more about chronic traumatic encephalopathy, how it affects the brain, and how SPECT scans may help clinicians recognize and address the condition before irreversible damage occurs.
Chronic Traumatic Encephalopathy is a progressive brain disease caused by repeated head injuries or repeated blows to the head. This includes concussions and subconcussive impacts. The repeated head injuries that cause CTE are common among certain populations, such as athletes.
Over time, these repeated head injuries damage brain cells and disrupt healthy brain function. Concerningly, CTE is associated with abnormal buildup of tau protein, which impedes communication between brain cells and eventually leads to cell death.
Traumatic brain injuries (TBIs) should always be taken seriously. However, CTE describes an extremely dangerous type of brain damage. Indeed, CTE is different than damage caused by single traumatic brain injury (TBI).
Examining whether CTE affects individuals with other types of TBIs, a study published in 2025 further established the link between CTE and repeated head impacts. The study found that CTE does not typically affect people with a single brain injury.
In this study, researchers examined 47 donated brains from individuals who sustained brain injuries in their lifetimes. Of these, seven people (about 15 percent) had CTE. Five of them had a history of repeated head impacts, including:
One individual with CTE had not suffered repeated blows to the head, but they had experienced two very serious brain injuries, occurring decades apart, before their death.
On the other hand, subjects without CTE had mixed histories. Some played sports, and some sustained a few head injuries. Others had single brain injuries. These findings support earlier studies that associated CTE with extensive, repetitive head impacts.
There are no specific symptoms that have been directly linked to CTE. However, in people who were confirmed to have CTE at autopsy, symptoms included changes in behavior, cognition, movement and mood. They may have experienced any of the following:
Behavioral changes
Issues in Cognition
Changes to Mood
Movement Problems
CTE disproportionately affects certain groups. For example, one study determined that among 202 deceased former American football players, an astounding 177 of them—or 87 percent—had neuropathologically diagnosed CTE.
These repeated brain injuries and CTE are associated with numerous brain health challenges. A 2023 study noted that CTE often coincides with cognitive impairment and progression to dementia.
This study found that, among brain donors with high-stage CTE who died from neurodegenerative disease, approximately 75 percent had late-onset dementia (diagnosed at 65 years or older). They died within 10 years of their dementia diagnosis.
Furthermore, almost three-quarters of these subjects (73.1 percent) had co-occurring neurodegenerative diseases. These include Alzheimer’s disease (45.4 percent), Lewy body disease (31.2 percent), and frontotemporal lobar degeneration (15.1 percent), which affects behavior, personality, and language skills.
At Amen Clinics, football players with repeated brain injuries have reported symptoms such as:
Related: Persistent Post-Concussion Symptoms
The brain is an incredibly complex organ, with 200 billion neurons (brain cells) and trillions of connecting fibers. But it’s also very soft and delicate, like softened butter—and the skull is designed to protect it.
The skull holds the brain in place with many sharp bony ridges. When the head is hit by an external force (or in forceful movements such as whiplash), the brain can get injured as it slams into these ridges and other parts of the skull. The result is a concussion.
The brain also contains tau protein, an essential component that provides the lattice-like structure of brain cells. Think of tau proteins, found inside brain cells, like train tracks, providing structure to help the cells clear any unwanted and toxic proteins.
Brain damage that stems from repeated injuries leads to a breakdown of tau, which then pierces through cell membranes and interferes with cell functioning. The resulting inflammatory response damages the brain. Through repeated head injuries, CTE develops.
Experts identified CTE cases as early as the 1920s. In those days, people labeled boxers as “punch drunk” to describe the effects of the head injuries they sustained throughout their careers. The athletes developed personality changes, psychiatric symptoms, memory issues, and behavior problems.
CTE symptoms affect athletes in other sports too—such as soccer and hockey, as well as military personnel. Victims of ongoing domestic violence or childhood abuse can also develop CTE.
We know that CTE is a progressive, degenerative disease. But the exact underlying mechanisms that lead to abnormal tau proteins are still being researched. (Abnormal tau proteins are also a key marker of Alzheimer’s, but research has found that they differ in their structure.)
In the past, CTE has been conclusively diagnosed only through the examination of autopsied slices of brain tissue. CTE cannot be detected in a blood test or other diagnostic measure. In other words, it could be diagnosed only after an individual dies.
However, the new edition of Diagnostic Imaging: Brain has confirmed that brain neuroimaging tools, including SPECT, can help detect the changes that suggest CTE development—while the patient is still living.
Here at Amen Clinics, we understand that mental health is brain health. Yet, in the field of psychiatry, medical experts rarely look at the organ being treated: the brain. Instead of simply observing clusters of symptoms, SPECT serves as a functional brain imaging tool that enables clinicians at Amen Clinics to view the underlying brain activity patterns of their patients.
SPECT stands for single photon emission computed tomography. As a nuclear medicine study, SPECT has been proven to reliably evaluate the brain’s regional cerebral perfusion (blood flow) and activity.
SPECT therefore allows clinicians to determine:
Though it’s a state-of-the-art brain imaging tool, the research using SPECT is vast, and it has been safely used for decades. SPECT has helped study:
Amen Clinics has successfully used SPECT to help treat psychiatric patients with complex cases. In many instances, it can change a client’s diagnosis as well as their treatment plan, therefore optimizing results.
SPECT differs from MRI, fMRI, and PET scans. While an MRI shows the physical anatomy or structure of the brain, SPECT shows blood flow patterns, which indicate how an individual’s brain works. SPECT is also more easily accessible, affordable, and comfortable for the client, while being more reliable than other kinds of scans.
Brain SPECT imaging helps clients and clinicians pinpoint the underlying factors behind a wide variety of mental health conditions and cognitive issues. It can help detect problems that play a role in mental health, including:
Now, experts know that SPECT can also be helpful in detecting the early brain changes that point to cases of chronic traumatic encephalopathy (CTE).
Diagnostic Imaging: Brain, Fifth Edition covers the fast-changing field of brain imaging. As an authoritative neuroradiology reference, it serves as an invaluable resource for neuroradiologists, general radiologists, and trainees in the medical field. The book offers updated information on more than 300 brain and central nervous system conditions.
The textbook confirms that functional neuroimaging tools like SPECT can detect chronic traumatic encephalopathy-associated patterns during life. This marks a major shift in the evaluation of football-related or “punch-drunk” dementia stemming from repetitive blows to the head.
Of course, Amen Clinics has been using SPECT to help identify signs of traumatic brain injuries for years. It holds the world’s largest database of functional brain scans and conducted the first and largest brain imaging studies on active and retired NFL players.
The textbook notes that autopsy confirmation remains the gold standard for definitive CTE diagnosis. But its acknowledgment of imaging markers—particularly tau-binding PET, SPECT, and diffusion MRI tract abnormalities in living patients—signals a significant advancement in clinical capability.
For the first time, frontline psychiatrists, neurologists, sports physicians, and brain injury specialists have authoritative documentation that such imaging tools can help CTE patients. SPECT can identify characteristic changes strongly suggestive of CTE before death—and before severe neurological decline.
Clinical data mirror the textbook’s findings. For example, measurable metabolic, perfusion, and white-matter network changes often emerge decades before individuals show symptoms. This shift transforms CTE from a condition recognized only after a life is over into one that can be monitored and mitigated during life.
Traditional structural imaging (CT and MRI) frequently appears normal in people with extensive concussion histories. In contrast, the advanced methods outlined in Diagnostic Imaging: Brain, Fifth Edition can reveal:
These imaging signatures represent a critical step forward because they allow for:
Earlier diagnosis is critical for cases of CTE because outcomes can be vastly improved with treatment. Let’s take a look at research conducted at Amen Clinics as an example.
Previously, Amen Clinics joined with scientists from major universities to conduct an extensive study on reversing brain damage (not specifically CTE) in former NFL players.
Subjects underwent cognitive testing and quantitative EEG studies, along with brain SPECT imaging, to assess blood flow patterns in the brain. All tests were completed before the treatment started and again at the study’s end.
Before treatment, the participants’ brain scans showed that more than 90 percent of the players had damage to multiple areas of their brains, especially in:
Participants underwent lifestyle-related treatments, such as weight loss if needed. They also supplemented with omega-3 fatty acids, a high-potency multivitamin, and other aids designed to support the brain.
By the end of the study, four out of five of the former players (80 percent) showed improvements, evident through cognitive testing and brain imaging. Blood flow in certain areas of the brain vastly improved—poor blood flow, like head trauma, is a key factor in brain aging.
The research serves as evidence that individuals with brain damage, and perhaps with CTE, can take steps to boost their brain function now.
The following lifestyle recommendations offer a great place to start:
Related: Fun Ways to Stimulate the Brain
Amen Clinics will continue to advance research and clinical applications of neuroimaging for at-risk groups for CTE. These include professional athletes, military service members, and survivors of repetitive head trauma.
Thanks to cutting-edge tools and continued research, there is true hope for individuals concerned about CTE. The encouraging news that SPECT can assist in earlier diagnosis and treatment for CTE equips healthcare experts to change brain health for the better.
“Autopsy remains the gold standard for definitive CTE diagnosis,” says Dr. Daniel Amen, founder of Amen Clinics. “But this is a huge step forward. For the first time, one of the premier medical imaging textbooks acknowledges that we can see CTE-related changes in living patients. If we can see it, we can treat it sooner, and change outcomes.”
Chronic traumatic encephalopathy (CTE) happens to individuals who have sustained repeated head trauma. Any person who has increased risk factors for CTE is vulnerable. This includes anyone who plays contact sports, survivors of long-term abuse, or individuals in the military.
SPECT imaging, used at Amen Clinics, can show CTE markers in still-living clients. Clinicians can use imaging tools to evaluate the CTE brain, including tau-binding PET, SPECT, and diffusion MRI tract abnormalities. These characteristic changes strongly suggest CTE before death and before severe cognitive decline.
With SPECT imaging, clinicians can see CTE-related changes in living clients. When these changes are observed, targeted treatments can begin sooner—and potentially change the outcomes for these clients.

When depression—or even the medications meant to help your symptoms of depression—start to chip away at things that bring you pleasure, it can be deeply upsetting. Indeed, depression can steal the pleasure and well-being you previously found in certain hobbies, relationships, and even your sex life.
If you’re experiencing depression, and you’ve noticed your sexual desire shrinking or your body reacting differently, it may have to do with your mental health condition and its treatment.
If you’re experiencing depression, and you’ve noticed your sexual desire shrinking or your body reacting differently, it may have to do with your mental health condition and its treatment.
Understanding depression’s associated negative effects on your sexual function is the first step toward regaining control of your mind, body, and sexuality.
As antidepressants are usually a first line of treatment for moderate to severe major depressive disorder, it’s equally important to be aware of the sexual side effects of antidepressants as well.
When you learn how depression and antidepressants can disrupt sexual function, it helps you to be a better advocate for yourself when getting care. You’ll be more likely to find treatment that addresses your depression without affecting such a vital and important part of your life.
In this blog, you’ll discover how depression and medication impact sexual function, and what you can do to minimize their effects.
While depression is often rooted in general feelings of sadness, it impacts much more. Depression is associated with changes in your brain chemistry, energy levels, self-esteem, and motivation, too.
Cumulatively, these depression effects can blunt sexual desire and make intimacy feel like too much work. Research on mental health patients shows that those with more severe depression report significantly lower sexual drive.
In fact, a meta-analysis found a bidirectional relationship between depression and sexual dysfunction: depression raises the risk of sexual problems, and sexual dysfunction itself can increase the likelihood of depression.
So, if you’re experiencing low libido, difficulty becoming aroused, or trouble reaching orgasm, depression may be the culprit.
Sometimes trying to heal your mood can come with unintended costs. The sexual side effects of antidepressants may be more common than you think. People who take antidepressants may experience any of the following common side effects:
These challenges may persist while on the medication. In some instances, persistent sexual dysfunction lasts after stopping medication. Sexual side effects are largely determined by the type of antidepressant an individual takes.
For example, selective serotonin reuptake inhibitors (SSRIs) are commonly associated with sexual dysfunction, whereas bupropion (Wellbutrin) has low reported sexual side effects.
It’s important to discuss concerns about antidepressants and sexual side effects with your medical or mental health care provider. Of course, there are many natural treatments for depression to consider and discuss as well.
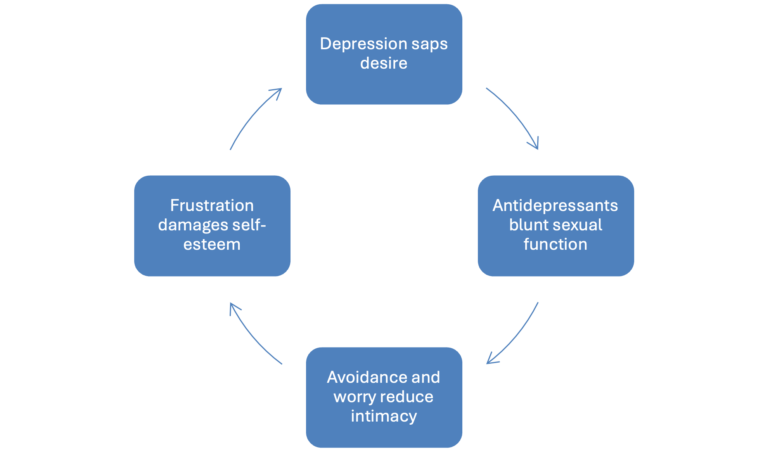
Unfortunately, sexual side effects can intensify symptoms of persistent low mood. What begins as a temporary dip in desire or arousal can turn into a repeating cycle: anxiety about sex, avoidance, relationship strain, and then guilt and shame—all of which can deepen depression.
Once this cycle begins, each factor feeds the others: depression saps desire; antidepressants blunt sexual function; avoidance and worry reduce intimacy; frustration damages self-esteem. And the loop continues.
Understanding how depression and antidepressants each uniquely impact brain function can help clarify why changes in sexual function happen, and why they matter.
With depression, neurotransmitters like serotonin, dopamine, and norepinephrine often shift. These neurochemicals regulate mood, but they also influence sexual desire, arousal, and reward. Lowered dopamine and norepinephrine, and imbalanced serotonin, can decrease the desire for intimacy and make sex feel uninteresting or exhausting.
Studies in depressed women show significantly lower sexual desire and reduced overall sexual functioning compared with their non-depressed peers. Moreover, depression brings fatigue, low self-worth, and emotional numbness. All of that can contribute to loss of interest in sex, even when someone is physically capable.
Antidepressants, especially SSRIs, work by increasing serotonin levels in the brain. That increase improves mood, but it can also interfere with sexual response. Research shows serotonin has an inhibitory effect on the neural systems that drive arousal, orgasm, and desire.
In particular, higher serotonin levels may lead to reduced dopamine signaling (important for desire), altered norepinephrine levels, or direct impacts on the neurological circuits that regulate sexual function.
That difference, between what depression does to your brain and what the medication does, helps explain why even when the depression lifts, the sexual side effects associated with antidepressants may linger or even intensify.
Here’s a real-world example shared by a happily married woman and patient of Amen Clinics. This woman went to see a traditional psychiatrist, where she complained of depressive feelings and an inability to sleep.
In less than ten minutes, the woman was diagnosed with depression and anxiety and was prescribed an SSRI (fluoxetine/Prozac), anti-anxiety medication, and a strong sleep aid.
She was feeling much better within a few days of taking the medication when something unusual and alarming happened. She was at a stoplight in her car when a man in the car next to her winked at her. She smiled at him then unbuttoned her shirt and revealed her breasts to the man.
Right after doing this, she was shocked and mortified by her out-of-character behavior. That’s when she quit taking the medications and came to Amen Clinics to seek out answers to help her understand her unusual behavior.
A comprehensive evaluation at Amen Clinics, including brain SPECT imaging, showed that the woman had low activity in her prefrontal cortex, which is commonly seen in ADHD. The antidepressant she was prescribed further reduced brain activity, leading to her impulsive sexual behavior. On a more targeted treatment plan, her depression improved without the impulsivity.
This story illustrates how easily a hasty, one-size-for-all prescription for antidepressants can result in unexpected behavior.
In this case, it appears to have increased impulsivity and a lack of inhibitions, especially around sex and intimacy. It’s a vivid reminder that sexual side effects aren’t only about desire or performance. Sometimes they impact identity, impulse control, and relationships.
Instead of guessing based on reported symptoms, emerging research using brain imaging, including single photon emission computed tomography (SPECT), suggests that observing images of brain activity and blood flow might provide a greater understanding of an individual’s brain function. And this could lead to more effective, targeted treatment plans for patients.
Using SPECT imaging at Amen Clinics, our clinicians have observed that depression and medications physically alter brain function in areas tied to mood, arousal, reward, and decision-making.
Interestingly, research indicates SSRIs can broadly alter neural activity in brain regions regulating sexual desire and arousal. For instance, research reveals a strong correlation between the binding affinity of an antidepressant to the serotonin transporter and reported sexual side effects.
Although imaging research specifically linking SPECT findings to long-term sexual dysfunction remains limited, such methods highlight how antidepressants rewire brain chemistry and alter neurotransmitter pathways.
At the same time, these insights pave the way for more personalized, brain-based interventions. By understanding someone’s unique brain activity, clinicians may in the future tailor treatments to support both mood and sexual health, a central philosophy at Amen Clinics.
SSRIs come with more than sexual side effects. In addition to low libido and potential for hypersexuality, side effects associated with SSRIs may include:
Experiencing even one of these side effects could be debilitating, negating any benefit the medication offers.
The cost of sexual dysfunction is great. It can negatively impact self-esteem and lead to frustration, anxiety, and anger. Hypersexuality, on the other hand, can cause psychological, relational, and even physical harm with a higher risk of sexually transmitted diseases.
Given these risks, SSRIs may not be right for everyone. As depressive disorders are the most common mental health disorders after anxiety in the U.S., it’s critical to have other effective medications and holistic alternatives for treating depression.
Thankfully, there are effective ways to treat depression that don’t compromise your sexual well-being. Healing shouldn’t have to come at the cost of intimacy. Being open and honest with your doctor is essential to finding a treatment approach that truly works for you.
You can choose an antidepressant with fewer sexual side effects. For example, as noted above, studies show medications such as bupropion (which works more on dopamine and norepinephrine) show a lower risk for sexual side effects.
When appropriate and under careful supervision, other non-serotonergic treatments may also be considered to preserve sexual function while treating depressive symptoms.
Natural supplements are a great alternative or adjunctive therapy to antidepressants. Consult an integrative or functional medicine practitioner to learn more as they typically are knowledgeable about herbal and nutritional supplements known to boost mood with few side effects. (Of course, any change to a treatment plan should be discussed with a medical doctor first.)
Saffron has been studied in placebo-controlled trials and found to improve mood without causing sexual dysfunction. In some cases, it even enhanced arousal and satisfaction.
Psychotherapy, sex therapy, and lifestyle interventions remain cornerstones in healing sexual dysfunction caused by medication and lifestyle choices. Working with a mental health professional (ideally one trained to address sexual function) can help unpack how depression, medication, self-esteem, relationship dynamics, and brain chemistry are interacting.
Lifestyle changes such as improving sleep, reducing stress, exercising, and nurturing emotional intimacy, can also help rebuild desire, arousal, and satisfaction.
Related: Antidepressant Withdrawal: What You Need to Know to Quite Safely
When depression is treated thoughtfully and under the guidance of a qualified mental health professional, you can continue to enjoy sexual intimacy or start to enjoy it again.
Sometimes, the missing piece isn’t a one-size-fits-all antidepressant, but a more comprehensive brain-based, personalized treatment plan.
Whether that means exploring alternative medications, integrating natural therapies, working with a therapist, or adjusting lifestyle habits, there are paths that support both mood and sexual well-being.
If you’re struggling, reach out to a qualified mental health professional who understands the complex interplay between mood, brain function, and intimacy. With clarity, compassion, and the right guidance, you can rekindle desire, strengthen connection, and reclaim this essential part of your life.
Depression, sexual dysfunction, and other mental health conditions can’t wait. At Amen Clinics, we provide personalized, science-backed treatment plans designed to target the root causes of your symptoms. Our 360-approach includes brain SPECT imaging, clinical evaluations, innovative therapeutic techniques, medications (when necessary), and holistic lifestyle recommendations to promote the health of your brain, body, and mind. Speak to a specialist today at 888-288-9834 or visit our contact page here.
No. While many antidepressants (especially SSRIs and SNRIs) are associated with a high risk of sexual side effects, others like bupropion, mirtazapine, and certain newer agents tend to carry a lower risk.
Depression influences neurotransmitters and brain circuits tied to desire, energy, reward, and self-esteem. The mood disorder itself, even without medication, often leads to reduced libido, lower arousal, and less interest in intimacy.
Some people find relief through lifestyle changes, psychotherapy, stress management, and supplements like saffron. While natural alternatives won’t replace medication for everyone, they may offer mood support without compromising sexual health. Just be sure to use them under guidance of a licensed doctor or therapist.
Oftentimes, yes. Clinics that use brain-based assessments—such as SPECT imaging at Amen Clinics—can better understand how depression and medications may be affecting a person’s brain function.
These insights can help to guide a personalized treatment approach that supports mood and sexual well-being with fewer or no sexual side effects depending on the treatment.