ARCHIVE
Men are more often associated with angry responses, but that doesn’t mean women don’t ever feel anger. From the ancient Greek tragedy murderess Medea to the impassioned protests spawned by the “Me Too” movement, female anger has famously erupted throughout the centuries. And, though anger can act as a positive force in human behavior, there are also times when anger overload—especially when it veers into the territory of intermittent explosive disorder (IED)—can become disruptive to everyday life. On the other hand, bottling up anger can be detrimental as well, causing symptoms of depression and other health problems, including addiction or difficulty in relationships. Left unchecked, anger can even play a contributing role in conditions such as ADD/ADHD, anxiety disorders, obsessive-compulsive disorder (OCD), bipolar disorder, and more. The good news is, there are healthy ways to express anger so it doesn’t erode health—and studies of the brain offer up some fascinating answers as to why women develop and process anger differently than men. Here are some surprising facts about female anger and the science behind it. Men are more often associated with angry responses, but that doesn’t mean women don’t ever feel anger… and studies of the brain offer up some fascinating answers as to why women develop and process anger differently than men.THE FEMALE BRAIN AND ANGER
Fact: Women’s brains reflect key differences that explain their unique anger responses.
When Dr. Jill Goldstein of Harvard Medical School used MRI scans to compare male and female brains, she found that women have larger volume in the frontal cortices and limbic cortices. As a reminder, the frontal cortex is involved in many higher cognitive functions, including language, judgment, planning, impulse control, and conscientiousness, while the limbic cortices are concerned with emotional responses. This might explain why women tend to be less impulsive and more concerned with emotions than men, as well as why their “busy” brains sometimes won’t stop worrying. It might also explain the source of the female brain’s key strengths, such as intuition, collaboration, self-control, and empathy. Brain imaging also shows that the hippocampus, one of the major memory centers in the brain, is larger in women. Men, on the other hand, have bigger amygdalas, the part of the brain that processes fear and anger, which may be why men often release those emotions in a crisis. With their larger prefrontal cortex (the area of the brain used to control anger and aggression), women are better at keeping strong negative emotions in check, research shows—possibly due to their ability to read others’ emotional cues and defuse tense situations. Also, the more empathic female brain may naturally respond to others’ distress with an instinct to calm the situation rather than display aggression. In fact, when a woman does turn aggressive, she’s more likely to initiate a verbal attack versus a physical one. But what about female anger that does lead to aggression? According to a study by the Amen Clinics team that utilized brain SPECT imaging, those who exhibit intense anger and outward aggression—men and women alike—show significant differences in brain activity, compared with non-aggressive individuals. They include:- decreased activity in the prefrontal cortex (linked to a lack of impulse control),
- increased activity in the basal ganglia and limbic system (associated with anxiety and depression), and
- temporal lobe abnormalities in the brain’s left region (seen with mood stability problems and aggression)
PMS, FERTILITY, AND ANGER
Fact: A woman’s cycle can dramatically affect the anger-related areas of her brain.
When we see the effects of PMS show up on brain scans, we know that PMS is more than just a hormonal issue—it’s actually a brain disorder. One patient at Amen Clinics, Jesse, visited after a fight with her husband. When she pulled out a knife to threaten him, he fled in fear. Jesse had long-standing temper issues, but they didn’t occur all of the time; they coincided with her menstrual cycle. Like clockwork, in the week before her period, Jesse would become moody, anxious, and aggressive—symptoms made worse by her habit of drinking too much alcohol. Jesse underwent brain SPECT imaging during the worst part of her cycle and then again two weeks later when she usually felt her best. The results were striking—the two sets of SPECT scans didn’t look like they even came from the same person! During the worst time of Jesse’s cycle, the brain scans showed overactivity in the “worry” region (the anterior cingulate gyrus) of her brain, but the judgment and impulse control part of her brain (the prefrontal cortex) was underactive (a state that was surely worsened by the alcohol). During the best-feeling time of her cycle, Jesse’s brain was much more balanced. The best solution for her was not just anger management therapy—she needed to stop drinking and get her hormonal fluctuations under control, too. After all, PMS symptoms arise when estrogen and progesterone levels sink to their lowest, while serotonin, the feel-good neurotransmitter, also falls. Prolonged anger over time may even have a negative impact on a woman’s fertility (a side effect that can also occur in men). Though infertility has many potential causes, one of the most common is stress. Being frequently upset, tense, or angry can clamp down on the fallopian tubes, making it harder to conceive, and research shows that chronic stress causes hormonal changes that disrupt reproductive function. In the same way that stress prematurely ages your body and skin, it also speeds up the aging of the reproductive system.CHANNELING ANGER FOR WOMEN
Fact: Anger can be a beneficial response—or severely detrimental to a woman’s daily life.
Anger, of course, can be helpful—and not only because keeping anger bottled up can backfire. One study, for example, found that those who fail to express their anger in a relationship are more likely to encounter issues over the long term. But studies have shown that expressing anger (when done in constructive, not destructive, ways), has many benefits. At its most basic, from early human times, anger has helped ensure our survival by alerting us to danger, propelling us to action, and sharpening our focus in times of fight-or-flight. Another study found that anger and risk assessment were associated with optimism and risk-taking, leading to more positive outcomes for those who experienced anger. On a deeper level, looking for the source of anger when it arises can point us toward issues that are calling for our attention. Ultimately, we find ourselves developing a healthier emotional intelligence as we show a willingness to embrace difficult emotions such as anger, rather than avoiding or repressing them. Simply approach your anger with curiosity, not annoyance, and treat this as an opportunity to learn and grow.COPING WITH FEMALE RAGE
Fact: Women can manage anger with several natural solutions.
Despite these potential positives, there’s no doubt that moderate levels of anger can have a negative impact on life. If that’s the case, there are many simple, natural ways to cope with it: You can try meditation and deep breathing exercises, play some soothing tunes or nature sounds, exercise, write in a journal, or simply take a time-out to calm the physical symptoms of stress, such as rapid heartbeat and shallow breathing. Also, be sure to note—and work on interrupting—any negative thinking patterns to help improve your mental well-being over time. When anger soars past the point of minor aggravation and into the territory of rage and/or violence, when it interacts in debilitating ways with other mental health conditions, or when you find that it’s impairing your relationships and daily activities, don’t hesitate to seek help. More serious underlying issues could be at work: a traumatic brain injury or other brain-related issues, exposure to toxins, or infections like Lyme disease. Brain SPECT imaging can help to determine the root cause, while treatments like therapy can help manage anger issues. What starts as a minor concern can, if left untreated, blossom into more intense expressions of rage or more serious conditions, so time is of the essence. Destructive anger issues, intermittent explosive disorder, and other mental health issues can’t wait. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, clinical evaluations, and therapy for adults, teens, children, and couples. Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here. Have you ever been friends with someone who is outwardly agreeable but then acts in ways that aren’t so kind? For example, let’s say you suggest going to a concert together and they enthusiastically agree. But when it comes time to buy the tickets they don’t respond to your messages. You go ahead and purchase them since they had initially said yes, but then your pal backs out at the last minute with a feeble excuse. Now you’re stuck with 2 tickets and have to scramble to find someone else to go to the show with you. Or consider this common office scenario. In a meeting, someone brings up an idea for a new project. Everyone verbally agrees with the plan, but when it comes time to get the project underway, one person procrastinates, doesn’t hit their deadlines, and effectively sabotages the whole thing. These are examples of passive-aggressive behavior. People who are passive-aggressive don’t express their anger, disagreement, or negative emotions directly, but rather through hostile or mean-spirited actions. These mixed messages leave others feeling confused, and this destructive trait can damage relationships at home, at work, or in love. People who are passive-aggressive don’t express their anger, disagreement, or negative emotions directly, but rather through hostile or mean-spirited actions. This can damage relationships at home, at work, or in love.WHAT IS PASSIVE-AGGRESSIVE PERSONALITY DISORDER?
Passive-aggressive personality disorder (PAPD) is not considered an official psychiatric diagnosis, but according to research published in the journal Psychiatry, some mental health experts contend that it should be. Within the field of psychiatry, PAPD has been viewed in a variety of ways, including a personality trait or syndrome, a dynamic behavioral pattern, or a negativistic personality disorder. Regardless of its classification, it is a real issue for many people that gets in the way of healthy relationships in all areas of life. Outwardly, passive-aggressive people seem pleasant, but internally, they feel frustrated, angry, or negative. They are often insecure, have low self-esteem, or are afraid people won’t like them if they voice disagreement. Research shows that people who are passive-aggressive have an increased risk of the following:WHAT CAUSES PASSIVE-AGGRESSIVE BEHAVIOR?
Experts point to both genetic and environmental factors in the development of passive-aggressive personality disorder. A study on twins in the Journal of Personality Disorders suggests that heritability accounts for 50% of a person’s risk for this trait. Several research papers have looked into the environmental factors that contribute to this personality type and concluded that the following increase a person’s risk:- Ineffective or harsh parenting
- Childhood trauma or abuse
- Neglect
10 SIGNS OF PASSIVE-AGGRESSIVE PERSONALITY DISORDER
How can you tell if you or someone you know has passive-aggressive tendencies? Here are 10 common behavior patterns associated with a passive-aggressive personality disorder.- The silent treatment: Passive-aggressive people may have a hard time discussing their anger or negative emotions, so they stop talking altogether as a form of punishment.
- Negative body language: Rolling the eyes or crossing arms while others are speaking can be indirect signs of disagreement, resentment, or frustration.
- Ghosting: Rather than ending a relationship—whether it’s with a romantic partner or a colleague—in person, the passive-aggressive type is more likely to ghost the other person. They simply refuse to communicate anymore to avoid conflict.
- Making excuses: Individuals who exhibit passive-aggressive behavior are experts at coming up with excuses to get out of doing things.
- Procrastinating: When the passive-aggressive person says yes to something they should have said no to, they will often put it off as long as possible.
- Forgetful: These people tend to forget tasks, assignments, or promises they made that they didn’t want to do in the first place.
- Being sarcastic: Individuals who are passive-aggressive frequently use sarcasm to subtly attack others while claiming they are “just kidding.”
- Blames others: Passive-aggressive types are quick to say that their shortcomings are due to the fault of others.
- Pouts or acts sullen: Saying things are “fine” while conveying a sour mood is a common trait among passive-aggressive people.
- Being a complainer: Whining or complaining about things without taking any positive actions to change things is common in this personality type.
HELP FOR PASSIVE-AGGRESSIVE BEHAVIOR
People with PAPD can get better. Recognizing the signs associated with this personality trait is one of the first steps. However, be aware that many of the signs listed above are similar to symptoms associated with other mental health issues, such as ADHD, anxiety, depression, bipolar disorder, conduct disorder, oppositional defiant disorder, schizophrenia, or substance use disorder. Ruling out these other conditions or identifying co-occurring disorders can be helpful in finding the right treatment. Solutions for a passive-aggressive personality disorder may include beneficial forms of psychotherapy, training to improve the ability to resolve conflicts directly, increasing self-esteem, overcoming negativity, and addressing any co-existing disorders. Personality disorders and other mental health issues can’t wait. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, clinical evaluations, and therapy for adults, teens, children, and couples. Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here. Post-traumatic stress disorder (PTSD) has earned a place in the social consciousness due to increased media coverage about the condition. If you’re like most people, you probably think PTSD predominantly affects military veterans. Wrong! Surprisingly, the #1 trigger of PTSD in the U.S. is rape. Statistics from the Anxiety and Depression Association of America shows that 46% of women and 65% of men who are raped will develop the disorder, which affects 7.7 million adult Americans. Other forms of sexual assault—including attempted rape, unwanted physical contact, and childhood sexual abuse—can also increase the risk of developing PTSD. If you’re like most people, you probably think post-traumatic stress disorder (PTSD) predominantly affects military veterans. Wrong! Surprisingly, the #1 trigger of PTSD is rape.HOW COMMON IS SEXUAL ASSAULT?
Sexual assault is alarmingly common. Every 68 seconds, someone in America is sexually assaulted, according to RAINN, the nation’s largest anti-sexual violence organization. And CDC statistics show that over 1 in 3 women and 1 in 4 men experience sexual violence in their lifetime. Experts agree that the incidence of sexual assault is likely much higher as many cases go unreported. The lack of reporting is due, in part, to the stigma attached to being a rape survivor. Victims often feel guilt and shame about the experience, so they keep it to themselves. In some cases, an abuser threatens the victim or their loved ones with physical violence if they tell anyone. In other instances, victims feel hopeless and think that telling someone will do no good. Still, others may fear that speaking up will invite unwarranted scrutiny and victim-blaming. Sadly, this means that millions of Americans keep rape and other forms of sexual assault a secret and don’t seek help for the distressing psychological consequences they bring.SEXUAL ASSAULT AND PTSD
Following sexual trauma, it’s common to experience feelings of stress, anger, fear, anxiousness, guilt, and sadness. For most survivors, these feelings subside over time, but in others, they fester into PTSD. The researchers behind the 2020 meta-analysis mentioned earlier suggest that the trauma associated with sexual assault can result in the dysregulation of the body’s stress response system, leading to chronic stress or PTSD. Sexual assault survivors are more likely to develop PTSD than people who experience other forms of trauma. An epidemiological study of over 4,000 women found that 32% of rape survivors and 31% of sexual assault survivors will have PTSD at some point during their lifetime. Compare that to just 9% of survivors of traumatic events, such as a car accident or natural disaster, that aren’t crime-related. Brain SPECT imaging, which measures cerebellar blood flow and activity, shows that PTSD is associated with overactivity in the emotional centers of the brain. This overactivity seen on SPECT scans typically looks like a diamond pattern that is also associated with an increased risk of other mental health issues.OTHER MENTAL HEALTH CONSEQUENCES OF RAPE
PTSD isn’t the only psychological fallout associated with rape and other forms of sexual assault. Being the victim of this form of trauma is also linked to a heightened risk of a range of psychiatric issues, including:Depression and anxiety.
Take a look at the findings of a 2019 study involving over 300 middle-aged women in JAMA Internal Medicine, for example. In this study, 22% of the participants said they had been sexually assaulted, and the survivors were 3 times as likely to experience symptoms of major depression and twice as likely to have anxiety.Suicidal thoughts and behaviors.
For some victims, the psychological impact of the incident is so powerful that they begin having suicidal thoughts. A 2020 meta-analysis of dozens of studies with over 88,000 participants found a significantly greater prevalence of suicidal thoughts and behaviors among people with a history of sexual assault compared with those who had no such experiences. Specifically, over 27% of sexual assault survivors experienced suicidality compared to just 9% of people with no history of assault. This analysis confirms earlier research indicating a rise in suicidality following sexual assault. For example, a study in the Archives of General Psychiatry indicates an increased risk of suicide attempts in women with a history of sexual assault. When the sexual trauma occurred before the age of 16, the rate of attempted suicide was 3-4 times higher. Increased suicide risk also affects teens. Troubling findings in JAMA Pediatrics point to an increased rate of suicide attempts among teenage females who have experienced recent dating violence and males who have been subjected to sexual assault.Addictions.
A wealth of research indicates that sexual assault and rape increase the risk of developing substance abuse. Experts suggest that sexual assault victims may turn to alcohol or drugs to cope with the psychological distress that typically follows an attack.Dementia and other brain disorders.
New brain imaging research from the University of Pittsburgh shows that not only does sexual assault impact mental health, but it can also harm brain health. This 2021 study in Brain Imaging and Behavior found that experiencing trauma, and especially sexual assault is associated with greater volumes of white matter hyperintensities (WMH), which are considered neuroimaging markers of dementia, cognitive decline, stroke, and other brain disorders.OVERCOMING PTSD ASSOCIATED WITH SEXUAL ASSAULT
If you’ve endured the trauma of a sexual assault and developed PTSD, it is possible to heal. In order to overcome PTSD related to rape—even if it occurred decades earlier—it’s critical to get a comprehensive assessment. SPECT can help you see if there are changes in blood flow or activity in the brain, such as the diamond pattern, that are typically associated with trauma and PTSD. Determining if you’re also suffering from other mental health issues—such as anxiety, depression, or substance abuse—is another critical part of the process to ensure you get the most targeted and effective treatment plan. PTSD, anxiety, depression, and other mental health issues can’t wait. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, clinical evaluations, and therapy for adults, teens, children, and couples. Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here. In recent years, researchers and health experts have recognized that anger, when used constructively, is an important, useful, and even beneficial emotion to well-being. It appears that anger, which can be destructive, also has a vital energy to it that motivates us to action, helps to improve communication in both personal and professional relationships, and promotes optimism, among other benefits. Yet, for many people, anger is a fraught emotion. It can be misused to dominate and intimidate others in both work and personal relations—while others deny they have any angry feelings at all, as it may be too uncomfortable or scary to feel them. Anger can facilitate greater cooperation and harmony in relationships. If the anger is justified, expressed constructively, and the response is appropriate, misunderstandings and conflict are often resolved. Anger is a powerful emotion that requires some skill to manage. On the one extreme, unchecked externalized anger can turn to violence and aggression; and on the other, repressed, internalized anger can cause depression, health problems, and communication difficulties. Somewhere in the middle, feeling and constructively expressing anger are essential and necessary to health and well-being. Let’s take a look at several ways anger helps you.6 SURPRISING BENEFITS OF ANGER
1. Anger Helps Us to Survive
Scientific research recognizes that anger has played an important evolutionary role in ensuring survival. Our primal “fight” response stems from anger. Anger motivates us to vigilantly detect threats and sharpens our focus. When our safety is at risk or we are attacked, our anger is automatically activated and drives us to defend ourselves, sometimes quickly and forcefully. Anger essentially alerts us when someone or something wants to hurt us and provides the aggression needed to overcome a stronger attacker.2. Anger Motivates Us
Researchers have discovered that anger is associated with what’s called approach-related motivation. They assert that there are two basic motivational forces that underlie all behavior—the impulse to approach, or move toward something desired, and the impulse to withdraw, or move away from unpleasantness. Approach motivation comprises emotions, cognitions, and actions that are driven by the wish to achieve desirable results. As it turns out, research shows that anger significantly activates the left anterior cortex of the brain, which is associated with positive approach behaviors. Conversely, emotions such as fear and sadness activate the right frontal cortex, which is tied to the more negative, withdrawal motivational system, marked by inhibition, timidity, and avoidance of some kind of punishment or threat. Thus, anger can potentially provide you with the energy that may be necessary to take action towards achieving certain goals or to correct difficult or unjust situations. Of course, the physiological arousal that happens with anger is motivating too—a quickened heartbeat and breath, as well as tense muscles. They prepare one to take critical action. A more passive or calm emotional state does not have the same impact on the body.3. Anger Gives a Sense of Control and Optimism
Anger provides us with a sense of control and corresponding optimism. Anger propels us to use our individual power, alone or collectively, to inflict costs or withhold benefits to get what we need. Individuals who constructively experience and express their anger are in a better position to fulfill their needs and control their destiny than those who suppress their anger. Harvard researcher Dr. Jennifer Lerner, who studies emotion and decision theory, found in one study that anger and risk assessment were associated with optimism and risk-taking, whereas fear was associated with pessimism and risk-aversion. Additionally, the study noted that angry people are more similar to happy people than fearful people in how they assess risk outcomes! Now that’s a surprise. In another study, Lerner examined Americans’ reactions to the terrorist attacks of 9/11 and discovered that angry feelings evoked a sense of clarity and control on a large scale, helping to reduce fear, ultimately allowing people to come together for a common cause. Interestingly, those who became angry were less prone to anticipate future attacks, while those who were fearful worried about future attacks. In short, when we are angry, we can feel more optimistic about our ability to change a particular situation. This empowers us to take action and move from an undesirable position to a desirable one.4. Anger Increases Cooperation
Anger can facilitate greater cooperation and harmony in relationships. If the anger is justified, expressed constructively, and the response is appropriate, misunderstandings and conflict are often resolved. The constructive expression of anger in personal relationships is healthy and necessary. It allows for greater emotional intimacy and/or cooperation. A study published in Society for Personality and Social Psychology determined that too quickly moving to forgiveness is not healthy, stating, “Sometimes expressing anger might be necessary to resolve a problem—with the short-term discomfort of an angry but honest conversation benefiting the health of the relationship in the long-term.” Conversely, failing to express anger in a relationship can be destructive, according to one research study. This can apply to all different types of relationships. Ultimately, expressing our anger constructively teaches people to respect us.5. Anger Can Lead to Self-Improvement
Anger can serve as an opportunity for spiritual and emotional growth. Anger can be an indication that there’s a deeper issue that needs to be addressed. A willingness to look at the source of our anger can be beneficial. Being both curious about and constructive in exploring our anger can provide insight into our faults and shortcomings, and lead to character development and greater self-esteem. One study examined how participants’ recent expressions of anger had impacted them. More than half of the 747 participants responded that getting angry ultimately led to a positive outcome, and a full third of them observed that their experiences of anger had provided useful insight into their own faults.6. Feeling Anger Expands Emotional Intelligence
Ultimately, having a willingness to embrace difficult emotions such as anger, rather than avoiding or repressing them, is a sign of emotional intelligence. When a person is emotionally intelligent, they do not resist anger, but instead, welcome it with curiosity and caution. Anger is potent, after all, and needs to be treated with care. People who practice this are more emotionally resilient as a result. One study observed that “people who prefer to feel useful emotions, even when they are unpleasant to experience, must understand emotions and seek to regulate them in strategic ways.” The study also asserted that those who tend to only want happy feelings do not exhibit the same level of emotional intelligence or resilience. There’s a benefit to feeling and dealing with the unpleasant aspect of anger.Working Through Anger
Science is still learning about how using our anger constructively helps us to be safe and healthy in the world. If you struggle with aggression and destructive anger or you have trouble expressing anger at all, talking to a mental health professional can help. Brain SPECT imaging can also provide valuable insights, as research shows that mild traumatic brain injuries can lead to aggression and violence in some people. Destructive anger issues, intermittent explosive disorder, and other mental health issues can’t wait. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, clinical evaluations, and therapy for adults, teens, children, and couples. Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here. At year-end 2019, the total prison population in the U.S. numbered a staggering 1,430,800. And of these prisoners, 8% were serving time for a violent offense, according to the Bureau of Justice Statistics. What makes some people violent? If you’re like most people, you may think it’s due to poor parenting, a character flaw, or just being a “bad” person. Brain imaging shows there may be another reason. Mounting scientific evidence shows that traumatic brain injury—even a mild one that doesn’t cause loss of consciousness—can lead to aggression or violent behavior in some people. Someone who has experienced a TBI may erupt with anger with little provocation. Something that seems inconsequential may set them off, and the severity of their reactions can range from irritability to verbal abuse to physical assault. Rather than writing off these individuals as bad people, it’s important to look at what’s happening in their brain. What makes some people violent? If you’re like most people, you may think it’s due to poor parenting, a character flaw, or just being a “bad” person. Brain imaging shows there may be another reason: head injuries.The Link Between Head Trauma and Aggression
Aggression following head trauma is more common than you might think. Research in The Journal of Neuropsychiatry and Clinical Neurosciences conducted a study in 2009 to evaluate 67 individuals who had suffered a TBI for the first time. Within 3 months of the injury, over 28% of them displayed post-TBI aggression (primarily verbal). In most cases, the aggression was associated with the onset of depression among other psychosocial problems. Among violent inmates, the prevalence of TBI is even higher. In a 2020 study in Frontiers in Psychiatry on violent offenders, over 77% reported experiencing one or more head injuries in their lifetime. Aggressive antisocial behaviors and substance use disorders were more common in those prisoners with a prior TBI. Other findings in The Journal of Neuropsychiatry found that people with intermittent explosive disorder, a condition associated with impulsive aggression, are significantly more likely to have experienced a mild TBI compared with healthy people or those with psychiatric disorders. Such was the case with a 5-year-old boy who stabbed 3 members of his family over a juice box. Although that case made national headlines, there are many more cases of domestic violence that go unreported and unseen. And expressions of violence can be quite frequent in some people. In a fascinating study in Brain Injury involving 46 people in a TBI neurobehavioral program, the researchers noted 3,914 acts of aggression over a two-week period. Of those acts, 443 were physical assaults while the rest were verbal.Post-TBI Self-Harm and Suicide
The violent behavior some people experience after a concussion isn’t always directed at others. In some cases, it manifests in the form of hurting oneself. Research in the American Journal of Public Health shows that head injuries increase the risk of suicide. And findings in a 2009 study reveal that self-harm is more prevalent in those with a prior head injury. Experts suggest that feelings of depression that emerge or worsen after a TBI can increase the risk of self-harm and suicidal behaviors.Related Consequences Associated with Head Injuries
A wealth of research shows that TBIs also increase the risk of depression, substance use disorders, ADD/ADHD, and more. These issues may indirectly contribute to violent behavior. For example, depressive symptoms are linked to an increase in the incidence of self-harm as you saw above. Drug or alcohol abuse impair thinking and judgment, increasing the chances of making poor decisions in relation to aggressive or violent behavior. ADD/ADHD, which is characterized by problems with impulse control, is associated with a tendency to act without thinking. Head trauma has also been linked to an increased risk of incarceration. In the U.S., 25-87% of all inmates say they have suffered a TBI compared with 25-38% in the general population.How Even Minor Head Injuries Negatively Impact the Brain
Brain SPECT imaging, a well-respected technology that shows how the brain functions, reveals that suffering a TBI can have serious impacts on the brain. Amen Clinics has built the world’s largest database of functional brain scans related to behavior—over 170,000 scans and growing. These SPECT scans show that head injuries decrease blood flow to important brain regions that have been damaged. Some brain areas that are commonly impacted due to head trauma include:Frontal Lobes
The brain’s frontal lobes are involved in impulse control, judgment, empathy, and more. When there is damage in this area it can increase the risk of aggression and violent behavior. Many people may think about committing violence or saying something abusive, but the vast majority of us work through the potential consequences of doing so and choose not to act out on those dark thoughts. When the frontal lobes are underactive, there’s a greater chance of acting out impulsively. In addition, decreased activity in the frontal lobes due to damage from a TBI is associated with a lack of empathy, meaning people don’t take others’ feelings into consideration. Instead, they blurt out hurtful things or lash out physically.Temporal Lobes
The temporal lobes, located on either side of the eyes and underneath the temples, are involved in mood, emotional stability, and learning. Abnormal activity in this important brain region is associated with temper problems, anger, and unpredictable moods and behaviors.Pituitary Gland
The pituitary gland is a pea-sized structure that lies in the back of the brain that is involved in hormone production. The pituitary gland sits in a bony area of the skull called the sella turcica, making it vulnerable to damage, especially from whiplash injuries. Damage to the pituitary gland can result in hormonal imbalances that increase the likelihood of a wide range of symptoms, such as anger, temper outbursts, depression, and more. Where’s the good news in all this? People who display aggression or act out violently may have a hidden brain injury. And there is hope for healing a damaged brain. When you put the brain in a healing environment, it can boost brain health and improve emotional stability and behavior. Violence, aggression, head injuries, and other brain health issues can’t wait. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, clinical evaluations, and therapy for adults, teens, children, and couples. Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here. With the onset of the “Me Too” movement in 2017, the extent of sexual abuse and harassment was brought onto the public stage. As notable celebrities and other high-profile people began to openly share their stories, it provided a forum for “everyday” people to also open up about their experiences of abuse. Being able to recognize they had the support of so many others created a greater sense of safety in talking about this far-too-common type of trauma that adversely affects millions and millions of people. Most of those who spoke about surviving sexual abuse were women. In fact, 1 out of every 3 women in the U.S. will experience some form of sexual violence during their lives. Although these statistics are staggering, what many people don’t know is that 1 in every 4 men will be subjected to sexual violence at some point in his life, with 1 out of every 6 boys being sexually assaulted before age 18. These men often suffer in silence due to feelings of shame or the stigma attached to such abuse.The Prevalence of Male Sexual Abuse
According to a report from the Division of Violence Prevention at the CDC, 25% of males targeted by sexual predators during childhood were raped before the age of 10, and another 25% between the ages of 11 and 17. Many more are molested. And, though people are often under the impression that sexual abuse is largely perpetrated by strangers, 90% of those who commit these heinous crimes are known to the child (or the family). Children are often groomed by those who target them, which among others, can be a coach, teacher, clergy member, neighbor, relative, or those who have befriended them through social media or gaming platforms.Men Often Don’t Disclose Their Sexual Abuse
It can be very difficult for men who were sexually abused as children—or even as adults—to talk about what happened to them. In a culture that promotes masculinity as being tough and resilient, it can be very uncomfortable for men to not only express the painful emotions and vulnerability related to sexual trauma, but also to see themselves as victims. What further complicates some of these terrible experiences—and can be psychologically confusing—is the automatic physiological sexual response that can occur, despite the trauma of the assault. It is often difficult for men who were sexually abused as children—or even as adults—to talk about the trauma of what happened to them. Quite often, boys and men who are sexually abused do not report the crimes against them. Feelings of shame and/or a sense of self-blame can make it very difficult for them to say anything to anyone. And some might try to talk about it but end up feeling invalidated if people they trust do not believe them or cannot understand how a male could be raped or forced to do something against his will. Because of this, boys and men might compartmentalize the experience and bury the painful memories of it.Coping Can Be a Challenge with Unprocessed Trauma
It’s not unusual for sexual trauma to lead to mental health problems such as depression, anxiety, PTSD, substance abuse, and/or difficulty controlling anger—especially when memories get triggered or they feel otherwise threatened. While not every survivor of unprocessed sexual trauma will struggle in life, many guys develop unhealthy coping mechanisms to help them manage the anguish and emotions about what happened to them. In addition to addiction mentioned above, these compulsive behaviors might include:- Workaholism
- Emotional eating
- Extreme sports or extensive physical exercise
- Sex and/or pornography addiction
- Self-harm, such as cutting or head-banging
Men Don’t Have to Suffer in Silence
If you’re a survivor of sexual trauma and have been keeping the painful memories to yourself, it’s important to know that there are experienced psychotherapists who can provide a safe environment for you to talk about what happened—a place where you will not be judged, but rather listened to and validated. Some therapists incorporate EMDR, which stands for eye movement desensitization and reprocessing, and is a method that can be very effective when working through trauma. There are also peer support groups for male survivors of sexual assault which can be very helpful. Groups like these help you to understand that you are not alone, and because they don’t have a hierarchy it can alleviate any concerns about a power differential when talking about your experience(s). After years of carrying the secret of their trauma, men often find that having a trusted person to help them work through their sexual abuse feels like a huge burden has been lifted from them. Recently, author and podcast host Lewis Howes talked with Dr. Daniel Amen about how life-changing it was for him when, 25 years after he was raped at age 5, he worked with a psychotherapist to process his trauma. Many men find that the more they are able to talk about what happened to them, the less control the memories have over them—and the more they are able to find healthy ways to cope as they move forward in their lives. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, clinical evaluations, and therapy for adults, teens, children, and couples Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here. Peer pressure is nothing new, especially among teens and adolescents. The influence peers wield on their social circle has long been associated with driving behavior—both good habits and bad habits. For example, seeing a friend drink, smoke, use drugs, bully others, or binge eat increases the likelihood of engaging in that behavior oneself. Experts call this “social contagion.” Sadly, it also applies to self-harm. This is especially alarming in light of the dramatic increase in self-injury among teens since the pandemic began. According to an analysis of healthcare claims by FAIR Health, claims for intentional self-harm as a percentage of all medical claims for adolescents aged 13-18 skyrocketed by 99.8% in April 2020 compared to April 2019. Experts suggest the number of teens engaging in nonsuicidal self-injury could continue to increase. Seeing a friend drink, smoke, use drugs, bully others or binge eat increases the likelihood of engaging in that behavior oneself. Experts call this “social contagion.” Sadly, it also applies to self-harm.WHAT IS NONSUICIDAL SELF-INJURY?
Nonsuicidal self-injury (NSSI) is the act of purposely harming oneself without the intention of taking one’s own life. People who hurt themselves often have a history of adverse childhood experiences, such as abuse, being bullied, childhood neglect, or sexual assault. They may turn to cutting, skin-picking, burning, or other forms of self-mutilation as a way to numb their emotional pain. NSSI is most frequently seen in adolescents and young adults. Research in Child and Adolescent Psychiatry and Mental Health indicates that 17% of adolescents report at least one incident of self-harm. That’s higher than the 15% of college students who say they have engaged in self-injury at least once, according to a 2011 study in the Journal of College Health. And it’s more than 3 times higher than 5% of adults reporting self-harm. Approximately 65% of those who engage in NSSI are female, but experts suggest the behavior is likely underreported in males.STUDY FINDS SELF-HARM IS SOCIALLY CONTAGIOUS
Long-standing research shows that among adolescents, exposure to a peer’s suicidal behaviors raises the chances of dangerous copycat actions. Newer findings in a 2020 Canadian study in Acta Psychiatrica Scandanavica indicate that having knowledge of a friend’s nonsuicidal self-injury is significantly associated with an adolescent’s own involvement with self-harm, suicidal thoughts, and suicide attempts. In this study, researchers administered the following 3 questions about NSSI and suicidal behavior to 1,483 Canadian adolescents ages 14-17.- In the past 12 months, did any of your friends deliberately harm themselves but not mean to take their life?
- Sometimes people deliberately harm themselves but they do not mean to take their life. In the past 12 months, did you ever deliberately harm yourself but not mean to take your life?
- In the past 12 months, did you ever seriously consider taking your own life or killing yourself?
SELF-HARM AND MENTAL HEALTH
A wealth of scientific evidence shows that NSSI is associated with other mental health conditions. Among people who engage in self-harm may also struggle with issues such as anxiety, depression, post-traumatic stress disorder (PTSD), borderline personality disorder, substance abuse, eating disorders, dissociative disorders, or obsessive compulsive disorder. The team of Canadian researchers also analyzed mental health status and its effect on NSSI, assessing any diagnoses for major depressive disorder, anxiety disorders, ADHD, oppositional disorder, or conduct disorder. They found that adolescents who met the criteria for an anxiety disorder or depression were more likely to say they knew a friend who had been involved in self-harming behaviors. Those with some form of anxiety—including certain phobias—ranked highest with 28.6% reporting knowing a friend who engaged in self-injury. Among teens with depression, 20.4% said they knew peers who tried to hurt themselves. Engaging in NSSI as an adolescent also has detrimental effects on mental health in adulthood, according to findings in a 2020 study in European Child & Adolescent Psychiatry. In this study, researchers followed students in grades 7-8 for 10 years. Compared to youngsters who did not engage in NSSI, those who repeatedly injured themselves as adolescents exhibited significantly higher rates of anxiety, stress, NSSI, and problems with emotional regulation a decade later.HELPING TEENS PREVENT OR HEAL FROM SELF-INJURY
Preventing and healing from self-harm is possible. Recognizing that NSSI is socially contagious is an important step in identifying an adolescent’s risk for self-injurious behaviors. Providing teens with strategies to handle peer pressure—for example, saying no like they mean it, disagreeing respectfully, or asking questions—can be beneficial in the prevention of this increasingly common problem. It is equally critical for parents to know the warning signs of self-harm, including scars, frequent cuts or bruises, far-fetched tales about how an injury occurred, wearing long sleeves even in summer, carrying sharp objects, declining academic performance, and social withdrawal. In addition, addressing any co-occurring mental health issues should be part of an NSSI treatment plan. Investigating brain health with functional brain imaging may also be beneficial as it can reveal underlying abnormal activity. A 2019 brain imaging study found decreased brain function in regions of the brain that play a role in emotional regulation. Finding solutions that enhance overall brain health and emotional well-being is key to overcoming nonsuicidal self-harm. Self-harm, suicidal thoughts and behaviors, and other mental health issues can’t wait. During these uncertain times, your mental well-being is more important than ever, and waiting until life gets back to “normal” is likely to make your symptoms worsen over time. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, remote clinical evaluations, and video therapy for adults, children, and couples. Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here. By Rishi Sood, M.D. Although there is a growing amount of research on and increased awareness about post-traumatic stress disorder, many misconceptions about PTSD persist.Here are 5 of the most common PTSD myths.
Myth #1. PTSD only affects military veterans.
PTSD and its effects on military veterans have been well documented, but other types of trauma are also known to cause the condition. For example, childhood abuse in the form of physical and sexual trauma is known to lead to PTSD. Children exposed to such trauma often struggle with mood regulation and have increased rates of self-destructive and suicidal behavior. PTSD can also occur later in life as a result of medical illnesses—such as myocardial infarctions, obstructive sleep apnea, or stroke—or due to stays in the intensive care unit, which many people have unfortunately experienced because of COVID-19.Myth #2. PTSD develops immediately after suffering a trauma.
Symptoms of PTSD can occur 3 months after a traumatic experience, but it often occurs much later. Delayed-onset PTSD describes a situation where an individual does not develop symptoms until 6 months after the inciting event. In some cases, individuals experience PTSD years later. In a study of World War II veterans, many reported experiencing such symptoms later in life. This was thought to be brought on by major life changes such as losing a spouse. Just because someone is not affected by a traumatic event soon after does not mean that the individual is immune from being significantly affected many years down the road.Myth #3. PTSD makes people violent.
Many individuals who experience PTSD do not display violent tendencies. In fact, many individuals with PTSD shut down and avoid situations that pose any perceived threat. This puts significant strain on personal relationships and the ability to effectively function at work. In the dissociative subtype of PTSD depersonalization and derealization are seen. Individuals who experience depersonalization feel disconnected from their body while individuals who experience derealization feel the world around them is not real.Myth #4. PTSD is just one thing.
Individuals with PTSD can vary significantly in their presentations. As a result of trauma, some individuals can develop externalizing symptoms, which are characterized by symptoms of aggression and impulsivity. To cope, many will turn to substances such as alcohol and marijuana to calm the brain. Unfortunately, this can lead to brain injury and can worsen focus and mood. Others may develop internalizing symptoms, which are characterized by somatic symptoms, anxiety, and depression. Individuals who were once extroverted and had a secure sense of self can become more isolated and distant.Myth #5. PTSD isn’t treatable.
Although PTSD can have devastating effects, the great news is that effective treatment is available. Psychotherapy can be an effective tool and there are different modalities utilized. Cognitive behavioral therapy (CBT), eye movement desensitization and reprocessing (EMDR), and other trauma-focused therapies can be helpful. In some cases, medications such as SSRIs or SNRIs can provide significant relief. MDMA-assisted therapy in a controlled clinical environment and in the presence of a trained therapy team is also being studied and appears promising.About the Author: Rishi Sood, MD, Amen Clinics New York
Dr. Rishi Sood practices at Amen Clinics, which offers in-clinic brain scanning and appointments, as well as mental telehealth, remote clinical evaluations, and video therapy for adults, children, and couples. Dr. Sood is board certified in Adult Psychiatry and Child and Adolescent Psychiatry. In addition to his background in psychiatry, he is a board-certified pediatrician. Find out more about our services at AmenClinics.com. On Wednesday, May 20, 1998, 15-year-old Kip Kinkel was caught with a stolen gun in his locker and suspended from school, pending possible expulsion. Police booked him on criminal charges and sent him home with his parents. According to Kip’s confession, his father was sitting at the kitchen counter drinking coffee while Kip grabbed a .22 rifle from his room then fired a bullet into the back of his dad’s head. When his mother arrived home later that day, Kip met her in the garage, told her he loved her, then shot her multiple times. The next morning, dressed in a long trench coat, Kip drove his mom’s Ford Explorer to a spot near Thurston High School and parked it. Carrying a rifle and two handguns, Kip walked down a hallway and into the school cafeteria, firing off over 50 rounds that killed two students and wounded about two dozen others. A group of classmates, including one teenager who had been shot in the chest, finally subdued him. After he was arrested and taken to the police station, the freckle-faced teenager lunged at an officer with a knife that he had strapped to his leg, yelling, “Kill me, shoot me.” The officer stepped back and used pepper spray on him. Kip was sentenced to 112 years in prison for aggravated murder and was prosecuted as an adult. Under Oregon law he was too young to face the death penalty. Kip had once been voted as “most likely to start World War III,” according to a Thurston High School student. Before the shootings, students at the high school said that Kip had talked about shooting people. After the shootings, officials found 5 bombs at the Kinkel residence, one of which went off when it was being disarmed. Authorities found a note in the living room that Kip wrote, saying: “My head just doesn’t work right. God damn these VOICES inside my head… I have to kill people. I don’t know why… I have no other choice.” What drives some people to kill another human being? Or to gun down dozens of their schoolmates? America has been captivated by killers for centuries—digging into their family histories, psychological profiles, and so much more. Now, thanks to brain SPECT imaging, we can also see inside their brains. What do brain scans reveal about murderers? America has been captivated by killers for centuries—digging into their family histories, psychological profiles, and much more. We use brain SPECT imaging to see inside their brains and have discovered 7 critical lessons. Amen Clinics, which has the world’s largest database of functional brain scans (over 160,0000 and growing), has scanned the brains of over 1,000 convicted felons, including over 100 murderers.Here are 7 lessons from the brain scans of murderers.
1. People who do the worst things often have troubled brains.
The brains of murderers typically don’t look healthy. Brain SPECT imaging is a technology that measures blood flow and activity in the brain. It shows 3 things: areas with healthy activity, areas with too much activity, and areas with too little activity. On SPECT, the brains of murderers show abnormal activity in a variety of brain regions, especially the prefrontal cortex involved with empathy, judgment, and forethought. Look at this scan of a healthy brain compared to a scan from Kip Kinkel.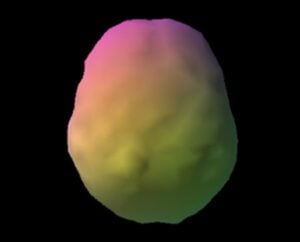

2. Murder does not always look the same in the brain.
You might think there is a singular pattern in the brain of killers, but there isn’t. Look at the brain scans of two 15-year-old murderers, for example. They look very different. The brain scan of Kip Kinkel shows underlying damage and toxicity and is dramatically underactive. In the SPECT scan of Paul, a teen who murdered his mother and 8-year-old sister with a baseball bat, it is evident that his brain works too hard.


3. Traumatic brain injuries are a major cause of psychiatric illness and violence.
Few people know about the link between traumatic brain injuries (TBIs) and mental health problems because most psychiatrists never look at the brain. TBIs are associated with an increased risk of violent behavior, including suicide and murder. According to research in The Journal of Neuroscience, the rate of aggression and violence after a TBI ranges from 35%-90%. The brain scans of several of the murderers scanned at Amen Clinics show underlying damage to the brain from past head injuries.4. Left temporal lobe abnormalities are common in violent people.
Many Amen Clinics patients who exhibited violence (murderers, arsonists, domestic assaults, rapists, bombers, etc.) had left temporal lobe abnormalities. The temporal lobes are located on either side of the brain behind the eyes and underneath the temples. Assault, murder, rape, arson, and other criminal behaviors are often associated with problems in this part of the brain. Other scientific research confirms that temporal lobe abnormalities are associated with increased aggression and violence.5. Traditional mental health care is failing.
A number of our nation’s most notorious mass shooters—including Kip Kinkel (Springfield, OR, 1998), Eric Harris (Columbine, CO 1999), Seung-Hui Cho (Virginia Tech 2007), James Holmes (Aurora, CO, 2012), and Nikolas Cruz (Parkland, FL, 2018)—had seen psychiatrists or mental health professionals and had received “standard of care” treatment before their crimes. The brain imaging work at Amen Clinics shows that cookie-cutter treatment plans for psychiatric illnesses don’t work. Not all brain types react the same way to psychotropic medications. For example, SSRIs, the most commonly prescribed antidepressants, are considered safe for many people. However, in some people with low activity in certain brain regions, they may increase impulsivity and behaviors that are out of character. Scientific research, including a 2017 study in BMJ, has shown that some antidepressants increase the risk of violence, suicide, and homicide, and the FDA issues a black box warning for antidepressants for people up to the age of 24. A growing body of neuroimaging research, including a 2020 study in the International Journal of Molecular Sciences and a 2019 study in The American Journal of Psychiatry, shows that brain imaging may help predict which patients will respond favorably to antidepressants.6. Murderous behavior based on brain problems can’t be fully excused.
Although brain dysfunction contributes to violence, it is not an excuse for bad behavior. People who commit heinous acts should not be excused and allowed to go home because they have a bad brain. Many people who have troubled brains never do anything bad. In judgment we must consider the brain. At this point in time, science shows that the brain is very important to moment-by-moment behavior, and it must be considered in sentencing people.7. Brains can be rehabilitated.
What if our society evaluated and treated troubled brains, rather than simply warehousing them in toxic, stressful environments? Based on over 30 years at Amen Clinics of helping patients enhance their brain health and improve their lives, it’s clear that our society could potentially save tremendous amounts of money by making a significant percentage of these people more functional. With better brain health, violent criminals who get out of prison are more likely to be able to work, support themselves, and pay taxes. The Russian author Fyodor Dostoyevsky once said, “A society should be judged not by how it treats its outstanding citizens, but by how it treats its criminals.” Instead of just crime and punishment, SPECT imaging teaches us that we should also be thinking about crime, evaluation, and treatment. Aggression, depression, anxiety, suicidal thoughts, and other mental health issues can’t wait. During these uncertain times, your mental well-being is more important than ever and waiting until life gets back to “normal” is likely to make your symptoms worsen over time. At Amen Clinics, we’re here for you. We offer in-clinic brain scanning and appointments, as well as mental telehealth, remote clinical evaluations, and video therapy for adults, children, and couples. Find out more by speaking to a specialist today at 888-288-9834 or visit our contact page here.The threat of illness, job losses, social isolation—it’s a recipe for heightened stress, irritability, and anger. But it’s even worse for people who are trapped at home with a domestic abuser.
Sadly, the coronavirus pandemic has created a sort of perfect storm for domestic violence. Reports of increases in partner abuse, child abuse, and pet abuse are emerging across the nation and around the world. According to a study in Forensic Science International: Reports, incidences of domestic violence have risen 40-50% in Brazil and are up 30% in France. In the U.K., the BBC reported that calls to the National Domestic Abuse helpline saw a 25% increase since the lockdown began. And in the U.S., hotlines are reporting a spike in calls.
Abusers often use tactics, such as isolation from friends and family, as a way to control their victims. Constant scrutiny, restrictions on behavior, and limiting access to necessities (like food and using the bathroom) are other common strategies. With the world on lockdown, this has given perpetrators a stronger weapon in their arsenal.
For victims, it’s made it more challenging to be able to reach out to friends or a support network for help without their abuser’s knowledge. And it’s preventing them from escaping the situation by leaving home when things turn violent. Going to a shelter may not be an option now for fear of infection from COVID-19.
This sad situation makes you wonder what makes some people violent? The answer lies in the brain.
Violence and the Brain
The added stressors of the coronavirus pandemic can be contributing to serious anger and violence issues. In some people, violent outbursts may be a sign of a mental health condition called intermittent explosive disorder (IED).
This condition is more commonly seen in people who grew up in an abusive home or in those who have suffered multiple emotional traumas. The likelihood of problems with anger or violent behavior is increased in people with other mental health problems, such as ADD/ADHD or personality disorders. In addition, conditions like anxiety, depression, or substance abuse are seen in over 80% of people who suffer from IED.
In a brain SPECT imaging study performed at Amen Clinics on people who had assaulted another person or damaged property, more than 70% had abnormalities in the left temporal lobe region of the brain. Brain imaging scans indicate that damage to the left temporal lobe or dysfunction in this area of the brain makes people more likely to struggle with irritability, anger, and violent thoughts and behavior.
The temporal lobes, situated on either side of the brain behind the eyes and underneath the temples, are involved with emotional stability, understanding and processing memories, and more. When there is abnormal activity in the temporal lobes, it can be associated with aggression (internally or externally directed), dark or violent thoughts, emotional instability, and other problems.
Temporal lobe problems can come from many sources, the most common being genetics, head injuries, and toxic or infectious exposure. Since the temporal lobes sit in a cavity surrounded by bone on 5 sides (front, back, right side, left side, and underside) they can be damaged by a blow to the head from almost any angle. In fact, the temporal lobes, along with the prefrontal cortex and the anterior cingulate gyrus, are the parts of the brain most vulnerable to damage by virtue of their placement within the skull.
Childhood Trauma and the Brain
For children, being abused or witnessing intimate partner violence can have devastating, long-term effects on the brain and mental health.
In a typical year, an estimated 4.5 to 15 million children experience exposure to physical violence at home. It’s likely that there will be an uptick in these numbers as a result of families being cooped up at home due to the pandemic. This doesn’t bode well for the future generation.
Research in a 2018 issue of JAMA Network Open found that for children, witnessing domestic abuse can cause the same damaging effects as if they had endured the abuse themselves. In addition, brain imaging studies show that childhood trauma—including physical, verbal, and sexual abuse—causes structural changes in the brain that have been linked to a greater risk of mental illness and addictions. For example, a 2016 review of neuroimaging studies in the Journal of Child Psychology and Psychiatry, and Allied Disciplines found that youngsters exposed to abuse experience physical changes in the following areas of the brain:
- Hippocampus: Decreased size in this area that is involved in memory and learning
- Prefrontal cortex: Reduced volume in this region, which plays an important role in impulse control, judgment, planning, and follow-through
- Cerebellum: Less-than-normal volume in this region located at the back of the brain that helps coordinate physical movement and thoughts
- Amygdala: Heightened activity in this area, which is known as the brain’s “fear center”
These brain changes can lead to trouble in many areas of a person’s life, including at school, at work, and in relationships.
Damaged Brains Can Heal
Domestic violence can seem like a hopeless situation with no way out. But decades of brain imaging work and clinical practice at Amen Clinics have shown that there is hope for people in abusive relationships and for children who have suffered emotional trauma. Addressing underlying brain dysfunction is critical to treating IED, as well as for overcoming the lasting consequences of experiencing or witnessing abuse.
Note: If you or a loved one is in an unsafe domestic situation, also consider these resources:
- In an emergency: call 9-1-1
- National Domestic Violence Hotline: 800-799-7233
If you’re struggling with issues that stem from growing up in an abusive family or you’re experiencing domestic violence, Amen Clinics can help. At Amen Clinics, we can help you—and everyone in the family unit—achieve better brain health and a stronger, more fulfilling relationship. During these uncertain times, your mental well-being is more important than ever, and waiting to get treatment until the pandemic is over is likely to make your symptoms worsen over time.
At Amen Clinics, we’re here for you. We offer mental telehealth, remote clinical evaluations, and video therapy for adults, children, and couples, as well as in-clinic brain scanning to help our patients. Find out more by speaking to a specialist today at 888-288-9834. If all our specialists are busy helping others, you can also schedule a time to talk.